
Abstract
The prescribing information for sildenafil citrate (VIAGRA, Pfizer, New York, NY, USA) recommends flexible dosing (50 mg initially, adjusted to 100 or 25 mg based on effectiveness and tolerability) in most men with erectile dysfunction (ED). In many men, however, 100 mg may be the most appropriate initial dose because it would reduce the need for titration and could prevent discouragement and treatment abandonment should 50 mg be insufficient. Results of two previously published double-blind, placebo-controlled sildenafil trials of similar design except for a fixed-dose vs flexible-dose regimen were analyzed. Relative to the flexible-dose, approximately one-third more men were satisfied with an initial and fixed dose of 100 mg. In addition, tolerability was similar, and improvements from baseline in outcomes on validated, ED-specific, patient-reported questionnaires were either similar (erectile function and the percentage of completely hard and fully rigid erections) or greater (emotional well-being and the overall sexual experience). The similarity in outcomes is not surprising given that almost 90% of the men in the flexible-dose trial titrated to 100 mg after 2 weeks. These data suggest prescription of an initial dose of 100 mg for men with ED, except in those for whom it is inappropriate.
Similar content being viewed by others
Introduction
For most men with erectile dysfunction (ED), the prescribing information for sildenafil citrate (VIAGRA, Pfizer) recommends an initial dose of 50 mg, increased to 100 mg or decreased to 25 mg based on effectiveness and tolerability (flexible dose).1 However, 100 mg sildenafil produced optimal erection hardness (fully hard and rigid) in a substantial proportion of men with ED.2 In addition, in dose-optimization studies3, 4 and at the end of double-blind, placebo-controlled (DBPC) treatment in recent reports of flexible-dose trials,5, 6 100 mg was the dose that was used by most men. Thus, the 100-mg dose may provide some additional benefit beyond that achieved with the 50-mg dose and may be the most appropriate choice for initiation of therapy in many men.
This report assesses erection hardness, erectile function, emotional well-being, satisfaction (disease related and treatment related) and the overall sexual experience in men treated with 100 mg fixed-dose sildenafil and in men treated with flexible-dose sildenafil (50 and 100 mg), using data from two DBPC trials that were similarly designed except for a fixed-dose vs flexible-dose regimen.7, 8 The objective was to assess the efficacy and tolerability of an initial dose of sildenafil 100 mg relative to the flexible-dosage regimen recommended in the prescribing information.
Materials and methods
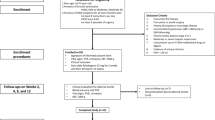
One trial was a multinational (Republic of Korea, Russian Federation, Spain and Sweden), parallel-group, randomized (1:1:1) DBPC trial of fixed-dose sildenafil (50 or 100 mg) or placebo administered on demand over an 8-week treatment period.7 The other trial was a multicenter (United States), parallel-group, randomized (1:1) DBPC trial of flexible-dose sildenafil (50 or 100 mg) administered on demand over a 10-week treatment period.8 In both trials, ⩽1 dose of study medication was to be taken per day. Details of the patients and methods of the two trials have been published previously.7, 8
As described previously,7, 8 several efficacy assessments were conducted, including the Erection Hardness Score (EHS9), the International Index of Erectile Function (IIEF),10 the Self-Esteem And Relationship (SEAR) questionnaire,11, 12, 13 the Sexual Experience Questionnaire (SEX-Q),14 the Quality of Erection Questionnaire,15 the Erectile Dysfunction Inventory of Treatment Satisfaction (EDITS)16 and three global efficacy assessment questions. Except for the global efficacy assessment questions, all assessment tools are validated, and a higher score indicates better outcome. Safety data included all adverse events (AE) reports from the original trials.
In this study, analyses were conducted on data from the intent-to-treat population for each study, which was defined as men who took at least one dose of study medication and who provided sufficient efficacy data for at least one efficacy analysis. Treatment effects were estimated using least square means from an analysis of covariance model for change scores from baseline to DBPC end of treatment on the IIEF, SEAR and SEX-Q, and the end-of-treatment EDITS Index score. The model used terms of baseline value, treatment group, investigator site and prognostic factors (age, ED duration, ED etiology) with P values calculated at the 5% significance level for the test of treatment group differences. Logistic regression (terms of treatment group, age, ED duration and ED etiology) was used to analyze the proportion of men who were satisfied with treatment (dichotomized EDITS score). The percentages of EHS 3, EHS 4 and EHS 3 or 4 erections based on all of the event log data since the previous visit were analyzed as clustered binomial data using a logistic regression (terms for baseline percentage, treatment group, age, ED duration and ED etiology), with a scale adjustment for overdispersion (estimated by Williams method) and model; treatment effects were estimated using predicted percentages from the model. Pearson correlations were computed between the SEX-Q change from baseline scores and all other outcomes (change from baseline or end of treatment); 95% confidence intervals for the correlation coefficient were constructed using Fisher's Z-transformation.
Results
Population and exposure
In both trials, each treatment group comprised ∼100 men, most of whom had ED that was of organic or mixed etiology and that was mild to moderate in severity (Table 1).
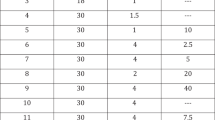
At week 2, 88% (92/104) of patients randomized to flexible-dose sildenafil and 92% (97/105) randomized to flexible-dose placebo increased their dose from 50 mg to 100 mg; at the end of the DBPC treatment, 87% (90/104) and 92% (97/105), respectively, remained on the higher dose. During the DBPC phase of each trial, patients in each treatment group received an average of seven or eight doses per month. Across both trials, only one man discontinued sildenafil (flexible dose) because of lack of efficacy and only two men discontinued sildenafil because of treatment-related AEs: moderate dyspepsia (100-mg fixed dose) and moderate headache (100-mg flexible dose).
Efficacy
Sildenafil, whether initiated at a fixed dose of 50 or 100 mg, or initiated at a dose of 50 mg and titrated as needed up to 100 mg, was significantly more effective than placebo (Table 2). The 100-mg fixed dose was significantly more effective than the 50-mg fixed dose in improving the IIEF Overall Satisfaction domain score; the SEAR Sexual Relationship Satisfaction domain, Overall Relationship Satisfaction subscale and Total scores; all SEX-Q domain scores; and the SEX-Q total score (Table 2). In addition, the EDITS Index was significantly higher in the fixed-dose sildenafil 100-mg group vs the fixed-dose sildenafil 50-mg group, although the difference between the dosage groups in the estimated percentage of men who were satisfied with sildenafil treatment (dichotomized EDITS scores: 93 vs 88%) was not statistically significant (Table 2).
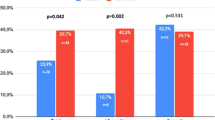
For the fixed-dose sildenafil 100-mg group relative to the flexible-dose sildenafil group (Table 2), there was a similar improvement from baseline in the percentage of EHS 4 erections (33 and 35%, respectively), EHS 3 or 4 erections (36 and 35%, respectively) and IIEF scores (⩽1 point difference between the groups across IIEF domains). However, for the fixed-dose sildenafil 100-mg group relative to the flexible-dose sildenafil group there was a greater improvement from baseline in SEAR scores (8–16 point difference between the groups across SEAR components) and in SEX-Q scores (3–7 point difference between the groups across SEX-Q domains), a greater least square mean±s.e. EDITS Index (78.4±2.0 and 66.5±3.3, respectively), and a larger estimated percentage of men who were satisfied with sildenafil treatment (dichotomized EDITS scores: 93 vs 69%). The SEX-Q total score, which assesses the sexual experience overall in the domains of erection, individual satisfaction and couples satisfaction, correlated positively with all other outcomes in both trials (Table 3).
Safety
In both trials, most AEs were mild or moderate in severity. The most frequently reported AEs were flushing, dyspepsia, headache and nasal congestion in the fixed-dose trial, which occurred at similar frequencies in the sildenafil 50-mg and 100-mg groups, and flushing, headache, nasal congestion and dizziness in the flexible-dose trial (Table 4). No treatment-related serious or severe AEs were reported in the sildenafil arms.
Discussion
As reported previously, sildenafil, whether initiated at a fixed dose of 50 or 100 mg,7 or at a dose of 50 mg and titrated as needed up to 100 mg,8 was significantly more effective than placebo in the treatment of ED, and there were additional benefits to the use of 100 mg fixed-dose sildenafil compared with 50 mg fixed-dose sildenafil.8 Although definitive statements about the comparative efficacy of 100-mg fixed-dose sildenafil and the flexible-dose sildenafil regimen are limited by the fact that the regimens were not compared within a controlled trial and the protocols of the two trials collated herein were not identical, the results of the current collated report suggest that an initial dose of sildenafil 100 mg is at least as effective and well tolerated as an initial dose of 50 mg with the option to titrate as needed. Definitive statements about the comparative tolerability of 100-mg fixed-dose sildenafil and the flexible-dose sildenafil regimen are also limited by the collated nature of the data presented in this report, although the low rate of discontinuation because of treatment-related AEs suggests that both regimens are generally well tolerated. The results of the current report are generalizable to the population of men with ED.
For the 100-mg fixed-dose regimen relative to the flexible-dose regimen, there was a similar increase from baseline in the percentage of EHS 4 erections and EHS 3 or 4 erections, a similar improvement from baseline in IIEF scores, a greater improvement from baseline in SEAR scores and SEX-Q scores, and a higher EDITS Index; approximately one-third more men in the 100-mg fixed-dose vs the flexible-dose regimen were satisfied with their sildenafil treatment. The similarity in outcomes between the two regimens is not surprising given that almost 90% of the men who initiated treatment with flexible-dose sildenafil titrated to a dose of 100 mg after 2 weeks. The apparent difference in outcomes on the SEAR, SEX-Q and EDITS between the two regimens may represent cultural differences between the European and Asian population treated with 100 mg fixed-dose sildenafil and the US (mainly white) population treated with flexible-dose sildenafil. The SEAR, SEX-Q and EDITS assess health-related quality-of-life concepts, which are likely to be more susceptible to cultural differences than are more functional concepts, such as those assessed by the EHS and IIEF. Cultural differences on SEAR responses were published previously.13, 17
Given that almost 90% of the men who initiated treatment with flexible-dose sildenafil titrated to a dose of 100 mg after 2 weeks, initiating treatment with 100-mg sildenafil should greatly decrease the need for dose titration and, in those men for whom a dose of 50 mg might prove ineffective, may decrease the risk of discouragement and treatment abandonment because of inadequate dosing. The high proportion of men titrating to a dose of 100 mg supports earlier results, which showed that 100-mg sildenafil produced optimal erection hardness (fully hard and rigid) in a substantial proportion of men with ED2 and that 100 mg was the dose used by most men in dose-optimization studies.3, 4, 6 Several studies reported that titration to the highest well-tolerated approved dose and/or early dose optimization contributed to treatment success.6
Treatment optimization, which includes selecting the most appropriate dose, ‘…may promote treatment adherence and thus facilitate optimal patient outcomes.’6 Some patients who are prescribed sildenafil for ED in the clinical practice setting neither refill their initial prescription nor seek alternative therapies.18, 19 For example, an analysis of sildenafil use during the first 24 weeks of availability at a large health maintenance organization revealed that only 61% of patients filled a second sildenafil prescription within 3 months of their first prescription.20 In addition, in a large dose-optimization study in which sildenafil was initiated at a dose of 50 mg for 4 weeks according to the package instructions, 14% (153/1109) failed to return for the second visit for scheduled dosage optimization.6 In several studies, incorrect administration, including suboptimal dosing, was the most frequent cause of nonresponse to sildenafil.6
An initial dose of sildenafil 100 mg may not be appropriate in some men. For example, higher plasma concentrations of sildenafil than those seen in healthy young volunteers occurred in men aged >65 years, in those who have hepatic impairment (for example, cirrhosis) or severe renal impairment (for example, creatinine clearance <30 ml min−1), and in those using concomitant potent cytochrome P450 3A4 inhibitors (for example, ketoconazole, itraconazole, erythromycin, saquinavir).1, 21, 22, 23 Because ritonavir greatly increased the systemic level of sildenafil in a study of healthy volunteers not infected with the human immunodeficiency virus, it is recommended not to exceed a maximum single dose of 25 mg of sildenafil in a 48-h period.1, 23 In addition, men with left ventricular outflow obstruction (for example, aortic stenosis, idiopathic hypertrophic subaortic stenosis) and those with severely impaired autonomic control of blood pressure can be particularly sensitive to the actions of vasodilators, including sildenafil.1 When sildenafil is coadministered with an α-blocker, patients should be stable on α-blocker therapy before initiating sildenafil treatment, and sildenafil should be initiated at the lowest dose.1, 24
In conclusion, sildenafil in doses of 50 and 100 mg is effective for the treatment of ED, and both doses are generally well tolerated. An initial dose of sildenafil 100 mg appears to be at least as efficacious and well tolerated as an initial dose of 50 mg with the option to titrate to the optimal dose. Furthermore, an initial dose of 100 mg may reduce the need for dose titration and may prevent discouragement and treatment abandonment in men for whom a dose of 50 mg is insufficient. This suggests prescription of an initial dose of 100 mg, except in those for whom it is inappropriate.
References
VIAGRA. Full Prescribing Information, Sildenafil Citrate. Pfizer, Inc.: New York, NY, 2008.
King R, Juenemann KP, Levinson IP, Stecher VJ, Creanga DL . Correlations between increased erection hardness and improvements in emotional well-being and satisfaction outcomes in men treated with sildenafil citrate for erectile dysfunction. Int J Impot Res 2007; 19: 398–406.
Steidle C, McCullough A, Kaminetsky J, Crowley A, Siegel R, Deriesthal H et al. Early sildenafil dose optimization and personalized instruction improves the frequency, flexibility, and success of sexual intercourse in men with erectile dysfunction. Int J Impot Res 2007; 19: 154–160.
Jiann BP, Yu CC, Su CC, Huang JK . Rechallenge prior sildenafil nonresponders. Int J Impot Res 2004; 16: 64–68.
Lowy M, Collins S, Bloch MT, Gillman M, Lording DW, Sutherland P et al. Quality of erection questionnaire correlates: change in erection quality with erectile function, hardness, and psychosocial measures in men treated with sildenafil for erectile dysfunction. J Sex Med 2007; 4: 83–92.
McCullough AR, Carson C, Hatzichristou D . A prospective study of the beneficial effects of dose optimization and customized instructions on patient satisfaction with sildenafil citrate (VIAGRA) for erectile dysfunction. Urology 2006; 68: 38–46.
Loran OB, Stroberg P, Lee SW, Park NC, Kim SW, Tseng LJ et al. Sildenafil citrate 100 mg starting dose in men with erectile dysfunction in an international, double-blind, placebo-controlled study: effect on the sexual experience and reducing feelings of anxiety about the next intercourse attempt. J Sex Med 2009; 6: 2826–2835.
Jones LA, Klimberg IW, McMurray JG, Padula R, Tseng L-J, Stecher VJ et al. Effect of sildenafil citrate on the male sexual experience assessed with the Sexual Experience Questionnaire; a multicenter, double-blind, placebo-controlled trial with open-label extension. J Sex Med 2008; 5: 1955–1964.
Mulhall JP, Goldstein I, Bushmakin AG, Cappelleri JC, Hvidsten K . Validation of the Erection Hardness Score (EHS). J Sex Med 2007; 4: 1626–1634.
Rosen RC, Riley A, Wagner G, Osterloh IH, Kirkpatrick J, Mishra A . The International Index of Erectile Function (IIEF): a multidimensional scale for assessment of erectile dysfunction. Urology 1997; 49: 822–830.
Cappelleri JC, Althof SE, Siegel RL, Shpilsky A, Bell SS, Duttagupta S . Development and validation of the Self-Esteem And Relationship (SEAR) questionnaire in erectile dysfunction. Int J Impot Res 2004; 16: 30–38.
Cappelleri JC, Bell SS, Althof SE, Siegel RS, Stecher VJ . Comparison between sildenafil-treated subjects with erectile dysfunction and control subjects on the Self-Esteem And Relationship Questionnaire. J Sex Med 2006; 3: 274–282.
Althof SE, O'Leary MP, Cappelleri JC, Hvidsten K, Stecher VJ, Glina S et al. Sildenafil citrate improves self-esteem, confidence, and relationships in men with erectile dysfunction: results from an international, multi-center, double-blind, placebo-controlled trial. J Sex Med 2006; 3: 521–529.
Mulhall JP, King R, Kirby M, Hvidsten K, Symonds T, Bushmakin AG et al. Evaluating the sexual experience in men: validation of the Sexual Experience Questionnaire. J Sex Med 2008; 5: 365–376.
Porst H, Gilbert C, Collins S, Huang X, Symonds T, Stecher V et al. Development and validation of the Quality of Erection Questionnaire. J Sex Med 2007; 4: 372–381.
Althof SE, Corty EW, Levine SB, Levine F, Burnett AL, McVary K et al. EDITS: development of questionnaires for evaluating satisfaction with treatments for erectile dysfunction. Urology 1999; 53: 793–799.
O'Leary MP, Althof SE, Cappelleri JC, Crowley A, Sherman N, Duttagupta S . Self-esteem, confidence and relationship satisfaction of men with erectile dysfunction treated with sildenafil citrate: a multicenter, randomized, parallel group, double-blind, placebo controlled study in the United States. J Urol 2006; 175: 1058–1062.
Jiann BP, Yu CC, Tsai JY, Wu TT, Lee YH, Huang JK . What to learn about sildenafil in the treatment of erectile dysfunction from 3-year clinical experience. Int J Impot Res 2003; 15: 412–417.
McCullough AR, Barada JH, Fawzy A, Guay AT, Hatzichristou D . Achieving treatment optimization with sildenafil citrate (Viagra) in patients with erectile dysfunction. Urology 2002; 60: 28–38.
Harrold LR, Gurwitz JH, Field TS, Andrade SE, Fish LS, Jarry PD et al. The diffusion of a novel therapy into clinical practice: the case of sildenafil. Arch Intern Med 2000; 160: 3401–3405.
Muirhead GJ, Wilner K, Colburn W, Haug-Pihale G, Rouvieux B . The effects of age and renal and hepatic impairment on the pharmacokinetics of sildenafil citrate. Br J Clin Pharmacol 2002; 53: 21S–30S.
Muirhead GJ, Faulkner S, Harness JA, Taubel J . The effects of steady-state erythromycin and azithromycin on the pharmacokinetics of sildenafil in healthy volunteers. Br J Clin Pharmacol 2002; 53: 37S–43S.
Muirhead GJ, Wulff MB, Fielding A, Kleinermans D, Buss N . Pharmacokinetic interactions between sildenafil and saquinavir/ritonavir. Br J Clin Pharmacol 2000; 50: 99–107.
Kloner RA . Pharmacology and drug interaction effects of the phosphodiesterase 5 inhibitors: focus on alpha-blocker interactions. Am J Cardiol 2005; 96: 42M–46M.
Acknowledgements
These studies were funded by Pfizer Inc. Editorial support was provided by Deborah M Campoli-Richards, BSPHA, RPh, at Complete Healthcare Communications, Inc and was funded by Pfizer.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
Peter Ströberg is a scientific study/trial investigator for Pfizer. Jed C. Kaminetsky is a consultant/advisor for Pfizer and Slate Pharmaceuticals; a meeting participant/lecturer for Astellas, Auxilium, Boehringer Ingelheim, GlaxoSmithKline, Lilly, Pfizer, and Solvay; and a scientific study/trial investigator for Aeterna Zentaris, Astellas, Auxilium, Indevas, Lilly, Pfizer, Plethora Solutions, and Spectrum. Nam Cheol Park has nothing to declare. Evan R. Goldfischer is a consultant/advisor for Astellas; a clinical trial investigator for Amgen, Astellas, Bayer, GlaxoSmithKline, Indevus, Lilly, Johnson & Johnson, Merck, Novartis, Pfizer, Ortho McNeil, Sanofi, Schering-Plough, Schwartz, and Unimed; and a lecturer for Astellas, Auxilium, Bayer, GlaxoSmithKline, Indevus, Lilly, and Pfizer. Dana L. Creanga was a paid consultant to Pfizer in connection with the statistical analyses performed in this study. Vera J. Stecher is an employee of Pfizer.
Rights and permissions
This work is licensed under the Creative Commons Attribution-NonCommercial-No Derivative Works 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/3.0/
About this article
Cite this article
Ströberg, P., Kaminetsky, J., Park, N. et al. Hardness, function, emotional well-being, satisfaction and the overall sexual experience in men using 100-mg fixed-dose or flexible-dose sildenafil citrate. Int J Impot Res 22, 284–289 (2010). https://doi.org/10.1038/ijir.2010.17
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ijir.2010.17
Keywords
This article is cited by
-
Enhanced understanding of the relationship between erection and satisfaction in ED treatment: application of a longitudinal mediation model
International Journal of Impotence Research (2014)
-
Changes in sexual inhibition and excitation during PDE5I therapy
International Journal of Impotence Research (2014)
