
Abstract
The aim of this study was to analyze the effects of psychological intervention on blood pressure, health-related quality-of-life (HRQOL), and stroke prevalence in patients with hypertension among the Chinese working population. Cluster sampling was conducted in September 2013 at the Shaanxi Jinduicheng Molybdenum Group General Hospital (intervention group) and the Shaanxi Province Hancheng Mining Bureau General Hospital (control group). The intervention group received regular psychological intervention for 2 years, including cognitive, emotional, and behavioral interventions. HRQOL was measured with the Spanish Hypertension Quality of Life Questionnaire (MINICHAL). We analyzed the data from a total of 409 subjects. After 2 years of psychological intervention, systolic blood pressure (SBP) and diastolic blood pressure (DBP) in the non-anxiety subgroup, and the anxiety subgroup were lower than baseline levels and lower than those in the control group. Post intervention, the mental state, somatic symptoms, and total MINICHAL scores were significantly below baseline levels, and the stroke morbidity was lower than that in the control group. Post intervention, SBP, DBP, and the MINICHAL scores in the intervention group were lower than those in the control group. SBP, DBP, and the MINICHAL scores were lower in the intervention group after 1 and 2 years of psychological intervention, as compared with the control group. Long-term psychological intervention can thus be used as an adjunctive therapy for patients with hypertension among the Chinese working population to improve their blood pressure, HRQOL and stroke prevalence.
Similar content being viewed by others

Introduction
Hypertension is an important risk factor for cardiovascular and cerebrovascular diseases such as stroke and coronary heart disease.1 Indeed, many studies have found that anxiety, depression, and high blood pressure (BP) are closely linked with coronary heart disease, diabetes, and other chronic diseases.2, 3, 4 The increasing incidence of anxiety and depression in patients with hypertension per year suggests that they may be related to the incidence of hypertension. In turn, patients with hypertension are more prone to anxiety, which can lead to high BP, thus creating a vicious cycle that affects patients BP.5 This interaction between anxiety and hypertension may be related to the sympathetic nervous system and the hypothalamic-pituitary-adrenal axis.6
Hypertension negatively affects quality of life. For example, stroke, cardiovascular disease and kidney disease caused by hypertension may lead to a deterioration of health-related quality of life (HRQOL) and to increased rates of hospitalization and morbidity.7, 8 Furthermore, a study by Mena-Martin et al.9 has demonstrated that patients with hypertension have poorer HRQOL. Given that psychological intervention has been shown to improve BP and quality of life in patients with hypertension,10, 11 we sought to further investigate this relationship in a group that experiences particularly high levels of stress.
With the development of the social economy, occupational groups are more prone to anxiety and depression.12 The proportion of individuals with ideal BP in the working population is less than 1/3 in China.13 Studies of patients with hypertension in the Chinese working population have mainly focused on its prevalence and influencing factors. However, few studies have examined the effect of psychological intervention on BP and quality of life in patients with hypertension among the Chinese working population.
In this prospective cohort study, we conducted a 2-year follow-up of employees of two mines in China. We measured the effects of psychological intervention on their BP, HRQOL, and stroke prevalence and compared the results with those from a control group that did not receive intervention.
Methods
Participants
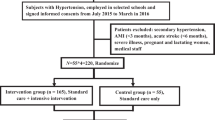
Between September 2013 and December 2015, 409 participants 18–50 years of age in the Shaanxi Province of China were recruited by general practitioners during a routine health check-up. The study was approved by the Institutional Review Board of the Fu Wai Cardiovascular Hospital (approval no. 2012–402, approval date, 17 July 2012) and was conducted according to the tenets of the Declaration of Helsinki and its revisions. All participants provided written informed consent to participate in the study.
Initial selection of participants
The cluster sampling method was used to select participants. We recruited professional employees from the Shaanxi Jinduicheng Molybdenum Group mine for the intervention group and the Shaanxi Hangcheng Mining Bureau mine for the control group. All participants were recruited in September 2013 when they visited the Jinduicheng Molybdenum Company Employees Hospital and the Hancheng Mining Bureau General Hospital (which served each mine, respectively) for their annual physical health examination. Participants were included in the study if they were 18–50 years of age, had consistently received annual health examinations and were working mining staff (managers, clerks, and mine workers). After screening, the intervention group included 600 subjects, and the control group included 530 subjects. Eligible subjects were excluded if they did not provide written informed consent, retired within the 2-year experimental period, had incomplete data, and/or refused to accept the psychological intervention and follow-up. After this standard exclusion, the intervention group comprised 592 subjects, and the control group comprised 526 subjects. Thus, the initial study group consisted of professionals working in a relatively closed mining area: the two mining areas were selected because they were expected to have minimal staff turnover during the 2-year testing period, and their employees were subjected to regular annual medical examinations at the local hospital. These participants would, thus, be less likely than other working populations to withdraw from the study. The two mines were 180 kilometers apart, and therefore, the non-intervention mining staff was unlikely to hear about the interventions received by the intervention group.
Selection of patients with hypertension
The selected participants were assessed for hypertension at enrollment. Hypertension was diagnosed according to the 2010 Chinese Hypertension Prevention guidelines, on the basis of a systolic BP (SBP) of ⩾140 mm Hg or a diastolic blood pressure (DBP) of ⩾90 mm Hg or the administration of antihypertensive drugs 2 weeks before the start of the study.14 Finally, on the basis of hypertension diagnosis, the data from the intervention group, which included 224 (out of 592) patients with hypertension, and the control group, which included 185 (out of 526) patients with hypertension, were analyzed.
Psychological intervention
The patients with hypertension in the intervention group received psychological intervention, including lectures, telephone follow-ups, printed informational materials, and monthly face-to-face psychological counseling. Intervention methods15 were as follows: (1) cognitive intervention aiming to enhance understanding and knowledge of elderly patients with hypertension and to increase their treatment motivation; (2) emotional intervention aiming to help patients understand the important effects of negative emotions, such as anxiety, depression and fear, on the occurrence, development, treatment, and rehabilitation of hypertension. Patients also learned how to regulate their emotions by changing their attitude toward reality and tried to avoid negative emotions. Patients were also shown how to establish a positive coping style (such as through humor, sublimation, and compensation) to decrease or alleviate the negative effects of psychological stress; and (3) behavioral intervention aiming to correct A-type behavior (characterized by a strong sense of competition, hostility toward others, and being overly ambitious, tense and impulsive) by encouraging exercise, adoption of a low-salt diet, smoking cessation, and limiting alcohol intake. Patients were taught muscle relaxation and deep breathing techniques, among other tools. The therapists were general practitioners of local hospitals who were trained by psychiatrists.
Survey administration
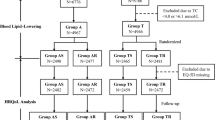
All hypertensive participants were followed-up for 2 years during visits to the local general hospital at 6 months,1 year, and 2 years after the initiation of the study. At all visits, the BP and HRQOL questionnaire responses were collected. The intervention group was also followed-up through monthly telephone calls to discuss their BP. Enrollment and the follow-up flow chart are shown in Figure 1.

Enrollment flow chart.
Questionnaire
HRQOL was measured with the Spanish Hypertension Quality of Life Questionnaire (MINICHAL). We chose the MINICHAL because it could be completed in a short time with a high response level and includes acceptable psychometric properties. MINICHAL is a multiple-choice 16-question questionnaire that assesses two factors: mental status (ten questions) and somatic manifestations (six questions). The MINICHAL also includes one question to assess patient perception of how hypertension and treatment have influenced quality of life. The patients answered questions according to the preceding 7 days. The answers were distributed in a Likert-type frequency scale with four answer options from 0 (no, not at all) to 3 (yes, very much). The maximum score for the mental status domain was 30, and for the somatic manifestations domain, it was 18. Thus, results closer to 0 (zero) indicated better quality of life. Question number 17, which assessed the patients’ overall perception of their own health, was also scored with the Likert scale, but was not included in either of the two domains.16, 17 The questionnaire is shown in Figure 2.

Spanish Hypertension Quality of Life Questionnaire (MINICHAL).
Physical examination
Blood pressure was measured using a standard mercury sphygmomanometer. The subjects were asked to rest for 5 min in the sitting position, after which the blood pressure in their right upper arm was measured twice, with the measurements at least 1 min apart. SBP and diastolic BP were recorded as phase I and V Korotkoff sounds. If the difference between the two measurements exceeded 5 mm Hg (1 mm Hg=0.133 kPa), the blood pressure was measured again. The average blood pressure was then recorded.
Outcome measurements
Outcomes in the intervention and control groups were assessed in terms of mean improvement in BP and HRQOL at 6 months, 1 year, and 2 years, as compared with baseline. All hypertensive patients from both groups were asked ‘Do you feel anxious?’ at the beginning of the study. If participants responded ‘yes’, then they were included in the anxiety subgroup; if they responded ‘no’, they were classified as the non-anxiety subgroup. Each subgroup was assessed for changes in BP relative to baseline. Some hypertensive patients were not taking medications for economic or other reasons. Therefore, hypertensive patients in the two groups were divided into subgroups as follows: medication and no medication. We then analyzed changes in BP in the medication plus psychological intervention subgroup, the simple psychological intervention subgroup within the intervention group, and the simple medication subgroup within the control group. In addition, we analyzed the stroke prevalence at the beginning and at the end of the study.
Statistical analyses
The data were entered in a double-entry manner using Epidata 3.1 software (Jens M. Lauritsen and Michael Bruus, Odense, Denmark). Continuous variables were expressed as the mean±s.d. The categorical data were expressed as numbers (%). Repeated measures ANOVA was used to assess BP and HRQOL, including the factors 'group' (intervention/control) and 'time period' (baseline and at 6 months, 1 year, and 2 years). Between-group comparisons of continuous variables were achieved with one-way analysis of variance followed by the Student–Newman–Keuls method. Between-group comparisons of categorical variables were achieved using the X2 test. The 2010 Sixth National Population Census data were used to standardize the data according to age. All the data were analyzed using SPSS 19.0 software. Two-sided P-values <0.05 were considered to be statistically significant.
Results
Baseline characteristics of the entire group
This study included a total of 409 hypertensive patients (n=224 in the intervention group and n=185 in the control group). Standardized by age, the overall prevalence of hypertension was 37.92%. Among the patients with hypertension, 307 were male (75.06%) and 102 were female (24.93%), and the mean age was 45.56±6.88 years. The average SBP was 142.20±18.95 mm Hg, and the average DBP was 91.83±13.12 mm Hg. Participants with hypertension in the two groups (intervention/control) did not differ in terms of sex, age, educational level, occupation, SBP, DBP, body mass index, or blood glucose and blood lipid levels at baseline (P>0.05). The results are presented in Table 1.
Effects of anxiety on BP in hypertensive patients before and after intervention in the intervention and control groups
Compared with the non-anxiety group, SBP and DBP levels were significantly higher in hypertensive patients who reported anxiety (P<0.05). After 2 years of intervention, the SBP and DBP of both the non-anxiety group and the anxiety group were significantly lower than baseline levels (P<0.05). In the control group, however, the SBP and DBP of the non-anxiety group did not change significantly (P>0.05), and the SBP and DBP of the anxiety group increased significantly (P<0.05) compared with baseline levels. The SBP and DBP in the anxiety subgroup, as compared with the control group, significantly decreased in the intervention group after 2 years (P<0.05). The results are presented in Table 2.
Effect of psychological intervention on the BP of patients with hypertension
In the intervention group, 119 patients with hypertension received antihypertensive drugs, and 105 patients with hypertension were not taking medication. In the control group, 38 patients with hypertension were treated with antihypertensive drugs. Whereas the SBP and DBP of the simple psychological intervention subgroup were decreased 2 years post intervention compared with baseline levels, the difference was not statistically significant (P>0.05). The SBP and DBP of the psychological intervention plus medication subgroup and simple drug subgroup were significantly lower at 2 years post-intervention compared with baseline (P<0.01). Compared with the simple drug subgroup, the psychological intervention plus medication subgroup displayed a more prominent decrease in SBP and DBP (P<0.05). The results are presented in Table 3.
Quality of life changes in patients with hypertension before and after intervention in the two groups
The HRQOL in patients with hypertension was measured using the MINICHAL. There were no significant differences in mental status, physical symptoms, or total MINICHAL scores between the simple psychological intervention subgroup, psychological intervention plus medication subgroup and simple medication subgroup at baseline (P>0.05). After 2 years, mental status, somatic symptoms, and total MINICHAL scores in the simple psychological intervention subgroup and the psychological intervention plus medication subgroup were significantly lower than baseline levels (P<0.05), and there were no significant differences between the two subgroups. In contrast, the mental status, somatic symptoms, and total MINICHAL scores increased over the 2-year period in the simple medication subgroup, but the difference was not statistically significant (P>0.05).The mental status, somatic symptoms, and total MINICHAL scores were significantly lower in the simple psychological intervention subgroup and the psychological intervention plus medication subgroup after 2 years, as compared with the simple medication subgroup (P<0.05). The results are presented in Table 4.
Effects of long-term psychological intervention on the BP and HRQOL of patients with hypertension
The BP and HRQOL at baseline, 6 months, 1 year, and 2 years were analyzed in patients with hypertension in the intervention and control groups. There were no significant between-group differences in BP or HRQOL at baseline or at 6 months (P>0.05). The BP and HRQOL of the intervention group was significantly lower than baseline (P<0.05) after 1 year of intervention. At 2 years, this difference was even more significant (P<0.01). The results are presented in Table 5 and Figure 3.

Effects of long-term psychological intervention on blood pressure and the HRQOL of patients with hypertension. *Significant change (P<0.05) in blood pressure and MINICHAL scores at the indicated time point relative to baseline as assessed by the Student–Newman–Keuls method. DBP, diastolic blood pressure; HRQOL, health-related quality of life; SBP, systolic blood pressure.
Effect of psychological intervention on stroke events in patients with hypertension
There were no significant differences in stroke prevalence between the intervention group and the control group at baseline (P>0.05). After 2 years, there was no significant difference in stroke prevalence in the intervention group, as compared with the baseline level (P>0.05), and the stroke prevalence was higher in the control group, as compared with the baseline level (P<0.05). Within-group comparisons showed that after 2 years, the stroke prevalence in the psychological intervention group was lower than that in the control group, but the difference was not statistically significant (P>0.05). The results are presented in Table 6.
Discussion
In this cohort study of 409 adults with hypertension, we examined BP and HRQOL over a period of 2 years. Our results showed that long-term psychological intervention improved the quality of life of patients with hypertension and decreased stroke prevalence. Although psychological intervention alone did not effectively reduce BP, when it was implemented in conjunction with drug treatment for hypertension, greater improvements in BP were observed. Thus, the present findings indicate that long-term psychological intervention can be used as an adjunctive therapy for patients with hypertension to improve their BP, quality of life, and stroke prevalence.
Smoking, obesity, family history, and excessive salt intake are widely accepted risk factors for the onset and progression of hypertension. The impact of psychosocial factors in the development and expression of hypertension is less clear. Many studies have shown that depression, anxiety disorders, and panic are risk factors for the onset and progression of hypertension.18, 19, 20 Other studies have shown that psychological factors are unrelated to high BP.21 In our study, BP was higher in people with anxiety. Although previous studies have shown that anxiety does not lead to high BP, most patients with hypertension lack understanding of their condition and prognosis. Consequently, they are plagued by doubt and worry about whether hypertension can be cured; this worry may stimulate the sympathetic nervous system and cause endocrine disorders and vasoconstriction, thus eventually leading to an increase in BP.6, 22 Therefore, we believe that anxiety increases the underlying causes of hypertension rather than directly leading to high BP. Furthermore, patients with hypertension are more prone to anxiety, which may increase BP. Thus, anxiety and hypertension promote each other, thus eventually leading to further increases of BP. Socio-economic development and intense competition mean that occupational groups are more prone to anxiety and other emotional disorders.23 Mine workers were chosen for the current study because their work environment is closed, and the work is monotonous; hence, we considered this population to be more prone to anxiety. Furthermore, a survey of workers from Hungary and Slovakia has found a high prevalence of hypertension in occupational groups.24 Related research has indicated that the prevalence of hypertension among the Chinese occupational population is also high.13 Therefore, our results suggest that attention should be paid to the relationship between occupational anxiety and hypertension. Active intervention to decrease the incidence of hypertension in occupational groups should be considered.
Increasing evidence suggests that non-pharmacological treatments, such as yoga25 and lifestyle modification26 can control hypertension. Psychological intervention has long been used in the treatment of disease. For example, psychological intervention can improve the prognosis of patients with cancer and decrease the occurrence of adverse cardiovascular events.27, 28 Although many studies have focused on patients with cancer and cardiovascular disease, the data on the effects of psychological intervention on BP are scarce. This study showed that psychological intervention improved BP in patients with anxiety-related hypertension, but only when implemented in conjunction with antihypertensive drugs. There are several possible explanations for this finding. First, psychological intervention may alleviate fear and anxiety toward a disease and build patient confidence to overcome it. Anxiety can be decreased by transferring patient attention so that patients may become less concerned about the disease. Second, anxiety and fear may result in distrust of the doctor, thereby leading to poor medication compliance. The decrease in anxiety and depression after psychological intervention may therefore improve patient trust in doctors and improve medication compliance and consequently may increase the efficacy of drugs. Third, case reports and retrospective studies have suggested that fat-soluble β-blockers are associated with anxiety and depression.29, 30 Hence, psychological intervention can improve patient compliance and the drug-induced side effects of anxiety and depression, thereby improving the efficacy of antihypertensive drugs. In conclusion, psychological intervention (alongside antihypertensive drugs) as a treatment for primary hypertension can serve as an important auxiliary measure to eliminate and prevent adverse psychological barriers, thereby regulating the nervous system, bodily fluids, and endocrine system, which are involved in hypertension. Our results showed that psychological intervention improved BP levels, whereas in the control group without psychological intervention, the BP level in patients with anxiety was significantly higher after 2 years. This result further indicates that psychological interventions may improve BP by decreasing patient anxiety. The benefit of psychological intervention on BP in patients with anxiety is shown by the decrease in BP in the intervention group and the increase in BP in the control group.
HRQOL has become increasingly important in clinical research over the past 15 years31 and has been extensively investigated in patients with hypertension. Hypertension is a major risk factor for cardiovascular disease and plays an important role in the development of stroke, myocardial infarction, heart failure, and renal failure, all of which lead to a deterioration of HRQOL.32, 33 This is the first study to use the MINICHAL for the measurement of HRQOL in adult patients with hypertension in China. Previous studies on HRQOL in patients with hypertension have focused on the factors influencing HRQOL34 or the relationship between hypertension and HRQOL.35 To our knowledge, this is the first study to investigate the effects of psychological intervention on the HRQOL in these patients in China. Our results showed that simple psychological intervention or psychological intervention plus medication significantly improved the HRQOL of patients with hypertension. Psychological intervention may therefore serve as a non-drug therapy that helps patients understand the psychological and social factors involved in hypertension, the important role of treatment in stabilizing BP and limiting adverse health effects, thus ultimately decreasing the psychological and economic burden on patients. Psychological intervention also aims to correct A-type behavior, improve interpersonal communication, and promote social function, and thus, it may also positively affect social relationships, another important aspect of quality of life.
Few previous studies have investigated the long-term and short-term effects of psychological interventions on disease. Our study revealed a difference in both the long- and short-term effects of psychological intervention on BP and HRQOL in patients with hypertension. There were no significant differences in BP or MINICHAL scores between the control group and the intervention group at 6 months. However, at 1 year, the BP and MINICHAL scores for the intervention group were better than those for the control group. At 2 years, these differences were even more significant. These results suggested that long-term psychological intervention may be helpful in improving BP and HRQOL in patients with hypertension. Hypertensive patients require not only long-term drug treatment but also long-term psychological intervention.
Stroke is the main cause of death in China, and the second largest cause of death worldwide.36 Hypertension is the primary risk factor for stroke.37 We observed a lower stroke prevalence in patients who received 2 years of psychological intervention. Thus, psychological intervention combined with drug therapy appears to effectively decrease BP and prevent the occurrence of stroke. Studies have not demonstrated the effects of psychological intervention on the incidence of complications in hypertensive patients. The results of the present study suggested that psychological intervention can decrease stroke prevalence in hypertensive patients.
This study has several limitations. First, anxiety was self-reported. Ideally, anxiety should be diagnosed and quantified with a scale, such as the Hamilton anxiety scale or the self-rating anxiety scale. Second, the effects of drugs cannot be completely ruled out. Owing to economic or other reasons, not all hypertensive patients take medications. Despite the separate analysis of drug factors (Table 3,Table 4), we still cannot rule out the effects of drugs on BP and stroke prevalence. Third, the participants were middle-aged; therefore, the findings may not apply to younger or older individuals. Fourth, the therapists were general practitioners of local hospitals and not psychiatrists. Therefore, the effects of psychological intervention may not have been fully realized. However, our study nonetheless indicates that psychological intervention has an effect on decreasing blood pressure in hypertensive patients. Fifth, our study population came from a relatively closed mining area with low staff turnover rates and, therefore, may not represent the general population.
In conclusion, our cohort study shows that long-term psychological intervention can be used as adjunctive therapy for patients with hypertension to improve BP and quality of life, and to decrease stroke prevalence in Chinese occupational groups. Therefore, drug treatment with complementary psychological intervention should be considered as an optimal treatment strategy for hypertension.
References
Roger VL, Go AS, Lloyd-Jones DM, Benjamin EJ, Berry JD, Borden WB, Bravata DM, Dai S, Ford ES, Fox CS . Executive summary: heart disease and stroke statistics—2012 update: a report from the American Heart Association. Circulation 2012; 125: 188–197.
Bhattacharya R, Chan S, Sambamoorthi U . Excess risk of chronic physical conditions associated with depression and anxiety. BMC Psychiatry 2014; 14: 1–10.
Holt RI, Phillips DI, Jameson KA, Cooper C, Dennison EM, Peveler RC . The relationship between depression, anxiety and cardiovascular disease: findings from the Hertfordshire Cohort Study. J Affect Disord 2013; 150: 84–90.
Carroll D, Phillips AC, Gale CR, Batty GD . Generalized anxiety and major depressive disorders, their comorbidity and hypertension in middle-aged men. Psychosom Med 2010; 72: 16–19.
Player MS, Peterson LE . Anxiety disorders, hypertension, and cardiovascular risk: a review. Int J Psychiat Med 2011; 41: 365–377.
Sobotka PA, Mahfoud F, Schlaich MP, Hoppe UC, Bohm M, Krum H . Sympatho-renal axis in chronic disease. Clin Res Cardiol 2011; 100: 1049–1057.
Maatouk I, Wild B, Herzog W, Wesche D, Schellberg D, Schöttker B, Müller H, Rothenbacher D, Stegmaier C, Brenner H . Longitudinal predictors of health-related quality of life in middle-aged and older adults with hypertension: results of a population-based study. J Hypertens 2012; 30: 1364–1372.
Lenski D, Kindermann I, Lenski M, Ukena C, Bunz M, Mahfoud F, Böhm M . Anxiety, depression, quality of life and stress in patients with resistant hypertension before and after catheter-based renal sympathetic denervation. Euro intervention 2013; 9: 700–708.
Mena-Martin FJ, Martin-Escudero JC, Simal-Blanco F, Carretero-Ares JL, Arzua-Mouronte D, Herreros-Fernandez V . Health-related quality of life of subjects with known and unknown hypertension: results from the population-based Hortega study. J Hypertens 2003; 21: 1283–1289.
Johnston DW . Psychological interventions in cardiovascular disease. J Psychosom Res 1985; 29: 447–456.
Abgrall-Barbry G, Consoli SM . Psychological approaches in hypertension management. La Presse Médicale 2006; 35: 1088–1094.
Niedhammer I, Malard L, Chastang JF . Occupational factors and subsequent major depressive and generalized anxiety disorders in the prospective French national SIP study. BMC Public Health 2015; 15: 1–11.
Rui G, Zeng-wu W, Xin W, Lin-feng Z, Zuo C, Min G, Ye T, Lan S, Man-lu Z, Run-lin G . Hypertension prevalence for working population in several provinces in China. Chinese Circ J 2014; 29: 172–175.
Liu L . Guidelines for the prevention and treatment of hypertension in China 2010. Chinese J Cardiol 2011; 39: 701–708.
Seligman MEP, Steen TA, Park N, Peterson C . Positive psychology progress. Am Psychol 2005; 60: 410–421.
Badia X, Roca-Cusachs A, Dalfó A, Gascón G, Abellán J, Lahoz R, Varela C, Velasco O . Validation of the short form of the Spanish hypertension quality of life questionnaire (MINICHAL). Clin Ther 2003; 24: 2137–2154.
Schulz RB, Rossignoli P, Correr CJ, Fernández-Llimós F, Toni PM . Validation of the short form of the Spanish hypertension quality of life questionnaire (MINICHAL) for Portuguese (Brazil). Arq Bras Cardiol 2008; 90: 127–131.
Davies SJ, Ghahramani P, Jackson PR, Hippisley-Cox J, Yeo WW, Ramsay LE . Panic disorder, anxiety and depression in resistant hypertension-a case–control study. J Hypertens 1997; 15: 1077.
Matthews KA, Katholi CR, McCreath H, Whooley MA, Williams DR, Zhu S, Markovitz JH . Blood pressure reactivity to psychological stress predicts hypertension in the CARDIA study. Circulation 2004; 110: 74–78.
Kayano H, Koba S, Matsui T, Fukuoka H, Kaneko K, Shoji M, Toshida T, Watanabe N, Geshi E, Kobayashi Y . Impact of depression on masked hypertension and variability in home blood pressure in treated hypertensive patients. Hypertens Res 2015; 38: 751–757.
Hildrum B, Romild U, Holmen J . Anxiety and depression lowers blood pressure: 22-year follow-up of the population based HUNT study, Norway. BMC Public Health 2011; 11: 2187–2198.
Lambert E, Dawood T, Straznicky N, Sari C, Schlaich M, Esler M, Lambert G . Association between the sympathetic firing pattern and anxiety level in patients with the metabolic syndrome and elevated blood pressure. J Hypertens 2010; 28: 543–550.
Wiegner L, Hange D, Björkelund C, Ahlborg G Jr. . Prevalence of perceived stress and associations to symptoms of exhaustion, depression and anxiety in a working age population seeking primary care-an observational study. BMC Fam Pract 2015; 16: 38.
Sonkodi B, Sonkodi S, Steiner S, Helis E, Turton P, Zachar P, Abrahám G, Legrady P, Fodor JG . High prevalence of prehypertension and hypertension in a Working Population in Hungary. American J Hypertens 2012; 25: 204–208.
Thiyagarajan R, Pal P, Pal GK, Subramanian SK, Trakroo M, Bobby Z, Das AK . Additional benefit of yoga to standard lifestyle modification on blood pressure in prehypertensive subjects: a randomized controlled study. Hypertens Res 2015; 38: 48–55.
Braith RW, Stewart KJ . Resistance exercise training: its role in the prevention of cardiovascular disease. Circulation 2006; 113: 2642–2650.
Rees K, Bennett P, West R, Smith GD, Ebrahim S . Psychological interventions for coronary heart disease. Cochrane Db Syst Rev 2011; 2: CD002902.
Andersen BL, Farrar WB, Golden-Kreutz D, Emery CF, Glaser R, Crespin T, Carson WE 3rd . Distress reduction from a psychological intervention contributes to improved health for cancer patients. Brain Behav Immun 2007; 21: 953–961.
Patten SB . Propranolol and depression: Evidence from the antihypertensive trials. Can J Psychiatry 1990; 35: 257–259.
Pollack MH . Comorbid anxiety and depression. J Clin Psychiatry 2005; 66 (suppl 8): 22–29.
Tchicaya A, Lorentz N, Demarest S, Beissel J, Wagner DR . Relationship between self-reported weight change, educational status, and health-related quality of life in patients with diabetes in Luxembourg. Health Qual Life Out 2015; 13: 1–9.
James PA, Oparil S, Carter BL, Cushman WC, Dennison-Himmelfarb C, Handler J, Lackland DT, LeFevre ML, MacKenzie TD, Ogedegbe O, Smith SC Jr, Svetkey LP, Taler SJ, Townsend RR, Wright JT Jr, Narva AS, Ortiz E . 2014 evidence-based guideline for the management of high blood pressure in adults: report from the panel members appointed to the Eighth Joint National Committee (JNC 8). JAMA 2014; 311: 507–520.
Soni RK, Porter AC, Lash JP, Unruh ML . Health-related quality of life in hypertension, chronic kidney disease and coexistent chronic health conditions. Adv Chronic Kidney D 2010; 17: 17–26.
Zhang Y, Zhou Z, Gao J, Wang D, Zhang Q, Zhou Z, Su M, Li D . Health-related quality of life and its influencing factors for patients with hypertension: evidence from the urban and rural areas of Shaanxi Province, China. BMC Health Serv Res 2016; 16: 277.
Korhonen PE, Kivelä SL, Kautiainen H, Järvenpää S, Kantola I . Health-related quality of life and awareness of hypertension. J Hypertens 2011; 29: 2070–2074.
Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker-Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez-Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez-Ruiz F, Perico N, Phillips D, Pierce K, Pope CA 3rd, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui-Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA . Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet 2012; 380: 2095–2128.
Meschia JF, Bushnell C, Boden-Albala B, Braun LT, Bravata DM, Chaturvedi S, Creager MA, Eckel RH, Elkind MS, Fornage M, Goldstein LB, Greenberg SM, Horvath SE, Iadecola C, Jauch EC, Moore WS, Wilson JA . Guidelines for the primary prevention of stroke: a statement for healthcare professionals from the American Heart Association/American Stroke Association. Stroke 2014; 45: 3754–3832.
Acknowledgements
This work was supported by the National ‘12th Five-Year’ science and technology support program ‘China's major cardiovascular disease investigation and key technology research’ (no. 2011BAI11B01), the Natural Science Foundation of China (no: 30871042), Shaanxi Province Science and Technology Research and Development Program International Science and Technology Cooperation and Exchange Project (no. 2012 kw-40-01) and Shaanxi Province Science and Technology Research and Development Plan of Natural Science Basic Research Program (no. 2014 JM2-8145).
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Liu, L., Li, M., Song, S. et al. Effects of long-term psychological intervention on blood pressure and health-related quality of life in patients with hypertension among the Chinese working population. Hypertens Res 40, 999–1007 (2017). https://doi.org/10.1038/hr.2017.80
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2017.80
Keywords
This article is cited by
-
Health-related quality of life in blood pressure control and blood lipid-lowering therapies: results from the CHIEF randomized controlled trial
Hypertension Research (2019)
-
The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019)
Hypertension Research (2019)
-
Clinical significance of stress-related increase in blood pressure: current evidence in office and out-of-office settings
Hypertension Research (2018)
-
Essential hypertension: the specialist as part of therapeutic intervention
Hypertension Research (2018)
