
Abstract
We investigated local pulse wave velocity (LPWV) in different aortic segments with respect to the rheological properties of the aorta with age-related progression of atherosclerosis in Kurosawa and Kusanagi-hypercholesterolemic (KHC) rabbits. Normal and KHC rabbits aged 10–12, 22–24 and 34–36 months were anesthetized with pentobarbital sodium (30 mg kg−1, intravenous). Pulse waves at the ascending aorta were recorded simultaneously with those at the proximal, middle and distal thoracic and abdominal aortas by moving a catheter with three micromanometers (40-mm intervals) at 80-mm intervals from the origin of the descending thoracic aorta. The aortic diameter was measured using an intravascular imaging system at the same aortic position at which the pulse waves were measured. LPWV was the greatest in the aortic arch, decreased gradually in the thoracic aorta and increased again in the abdominal aorta in KHC rabbits, whereas it was the lowest in the aortic arch, increased slightly in the thoracic aorta and increased gradually in the abdominal aorta in normal rabbits. LPWV increased significantly with age in most aortic segments. The change pattern of LPWV resembled that of the percent fractional lesioned area where LPWV was determined. The significant increase in LPWV with age was mainly due to the increase in the elastic modulus of the aortic wall with atherosclerotic progression as well as the increase in wall thickness. LPWV accurately detected the presence of atherosclerotic lesions and alteration in the rheological properties of the aortic regions through which pulse waves travelled.
Similar content being viewed by others


Introduction
Pulse wave velocity (PWV) has been widely used as a direct measure of arterial stiffness.1, 2 PWV has been well shown to increase with age3, 4, 5, 6 and with the progression of atherosclerotic lesions in humans7, 8 and animals.9, 10
Atherosclerotic lesions have been observed to develop in a favored aortic region such as the ascending aorta (AA) and areas around the orifices of branch arteries and progress toward the peripheral aortic sites with age in Kurosawa and Kusanagi-hypercholesterolemic (KHC) rabbits,11 while sclerotic lesions have been observed to develop mainly in the proximal abdominal aorta and spread peripherally with age in humans.12 Sawabe et al.13 reported that aortic PWV before death showed a significant positive correlation with the degree of atherosclerosis evaluated by autopsy examination in elderly patients. On the other hand, some investigators14, 15, 16 reported that PWV had no association with carotid intima-media thickening, one of the useful surrogate indices of the early stage of atherosclerosis. We previously reported that local pulse wave velocity (LPWV) in different aortic segments reflected extent and severity of the sclerotic lesions in young-adult KHC rabbits.17 Atherosmatous plaques have been shown to stiffen and develop toward the peripheral aortic regions with age in KHC rabbits in the previous studies.11, 18 It is advisable to measure PWV in a restricted aortic region, because this makes it possible to precisely detect age-related changes in arterial stiffness in different aortic segments.
In the present study, we investigated changes in LPWV in different aortic regions with progression of atherosclerotic lesions with respect to the alterations in the rheological properties of the aortic wall in KHC rabbits.
Materials and methods
Animals
Thirty normal and 30 KHC rabbits of both sexes aged 10–12, 22–24 and 34–36 months (n=10, for normal and KHC rabbits for any age group) were used in the present study. They were given a commercial diet (RC-4, Oriental Yeast, Tokyo, Japan) and raised in an air-conditioned, clean room at a room temperature of 22±2 °C, relative humidity of approximately 50% and light and dark cycle at 12L/12D. The present study was approved by the Experimental Animal Committee of Fukushima Medical University and was performed according to the Guidelines for Animal Care and Use of the US National Institutes of Health.
Serum biochemical assays
Blood was sampled from the posterior earlobe artery in the morning after overnight fastening. Serum was obtained by centrifugation at 3000 r.p.m. at 4 °C for 10 min. Serum total and high-density lipoprotein cholesterols, triglyceride and glucose levels were determined by enzymatic methods using an automatic analyzer (AU-5232, Olympus Corporation, Tokyo, Japan).
Surgical procedure and pressure wave recording
The surgical procedure was almost the same as that reported previously.17, 19 The rabbits were anesthetized with an intravenous administration of pentobarbital sodium (Nembutal; Abbott Laboratories, Chicago, IL, USA) at a dose of 30 mg kg−1 and were fixed in a supine position. Procaine chloride was applied to the incised regions to reduce pain. A catheter with a micromanometer at the tip (3Fr, SPS-330; Millar Instruments, Dallas, TX, USA) was introduced to the AA via the left common carotid artery. Another catheter with three micromanometers (3Fr, SPS-892; Millar Instruments) at the tip (40-mm intervals) was advanced to the distal end of the aortic arch via the left femoral artery. After stable blood pressure had been established approximately 30 min after the catheterization, pressure waves were measured simultaneously at four aortic positions: one in the AA and the others at the distal end of the aortic arch (position 0; P.0), proximal (P.1), middle (P.2) and distal (P.3) thoracic aortas and proximal (P.4), middle (P.5) and distal (P.6) abdominal aortas by carefully moving the tip of the catheter with three micromanometers from P.0 to P.4 at intervals of 80 mm. Pulse waves at these aortic positions were measured at almost the same mean arterial pressure (MAP) level before and after moving the catheter and were fed into a computer (PowerBook G4 M9691J/A; Apple, Cupertino, CA, USA) through an analogue-to-digital converter (PowerLab system 16s/, AD Instruments, Sydney, NSW, Australia) at intervals of 0.1 ms.
Measurement of intravascular ultrasound images
Pulsatile changes in the internal diameter (D) of the aorta were measured using an intravascular ultrasound (IVUS) imaging system (In-Vision Tsunami, EndoSonic Corp., Rancho Cordova, CA, USA). After pulse wave recording was completed, the catheter in the descending aorta was withdrawn, and an IVUS catheter (2.9Fr, 20 MHz, Eagle Eye Gold, Volcano Corp., Rancho Cordova, CA, USA) was advanced to P.1 from the left femoral artery. IVUS images were measured at P.1, P.4 and P.6 at almost the same MAP level as that when the pulse waves had been measured and were fed into a computer.
Determination of LPWV
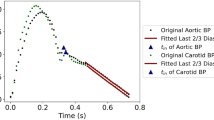
LPWV was determined as Δd/Δt, where Δd is the distance between two adjacent aortic positions and Δt is the difference in the rising point of the pressure waves between two adjacent aortic positions. The rising point of the pressure waves was defined as the peak of the second derivative of the original pressure waves, as reported previously.17, 19 The distance between AA and P.0 was calculated as D1−D2, where D1 is the distance between the micromanometer at AA and the entry site of the catheter in the left femoral artery, and D2 is the distance between P.0 and the entry site. D1 was measured at least twice in situ and was averaged after pulse wave measurement had been completed. Heart rate was calculated from the interval of rising point of pulse waves at AA.
Analysis of the rheological properties
The internal diameter of the aorta was measured using an IVUS catheter. Circumferential pressure–strain elastic modulus (Ep) was determined as Ep=PP/(Ds−Dd)/Dm, where PP is the pulse pressure and Ds, Dd and Dm were the systolic, diastolic, and mean ((Ds+Dd)/2) diameters at P.1, P.4 and P.6, respectively.17, 19, 20 The aorta was stored at −85 °C and thawed rapidly at 37 °C before the measurement of wall thickness. Wall thickness (h) in situ was estimated using the following formula: h=W/(1.06 × π × Dm × Wd), where 1.06, W, and Wd were the density of the wall,21 sample weight and sample width, respectively.
Determination of the percent fractional lesioned area (PFLA)
The aorta was excised from its origin to the bifurcation of the common iliac arteries, and the intimal surface of the aorta was xerox-copied. Monochromatic images were scanned and stored into a computer, after the outlines of the atheromatous plaques and the aorta had been carefully traced. The aortic surface was divided into seven aortic segments by the eight aortic positions at which pulse waves were measured; AA–P.0, P.0–P.1, P.1–P.2, P.2–P.3, P.3–P.4, P.4–P.5 and P.5–P.6, which were located in the aortic arch, proximal, middle and distal thoracic aortas and proximal, middle and distal abdominal aortas, respectively. The lesioned area at each segment was automatically selected and displayed in black with the Magic Wand Tool in Photoshop (Photoshop 6.0, Adobe Systems Inc, San Jose, CA, USA). The lesion-free area at each segment was displayed in white. PFLA at each aortic segment was calculated as a percentage of ratio of lesioned to entire areas in 10 KHC rabbits in each age group using the NIH Image software (Scion Corporation, Houston, TX, USA), as reported previously.17, 19
Statistical analysis
The data were analyzed with a three-level nested analysis of variance using a commercial statistical software (StatFlex version 6; Artech, Osaka, Japan). The difference between a pair of data was tested using the Scheffe’s multiple comparison test at each position if a significant difference was observed in the three-level nested analysis of variance. A value of P<0.05 was considered as significant.
Results
Serum lipid and glucose levels
Table 1 shows body weight, serum lipid and glucose levels in the normal and KHC rabbit groups aged 10–12, 22–24 and 34–36 months. There was little difference in body weight and glucose level between the KHC and age-matched control rabbit groups and among the three age groups in the two strains. Serum total cholesterol (P<0.001) and triglyceride (P<0.001) levels were extremely high in the KHC rabbit group compared with those in the age-matched control group, while high-density lipoprotein cholesterol (P<0.001) was significantly lower in the KHC rabbit group than in the age-matched control group.
Pathological findings of the atherosclerotic aorta in the KHC rabbit group
Figure 1 illustrates photocopies of the intimal surface of the aorta in the KHC rabbits aged 12, 24 and 36 months (a) and age-related change in PFLA at different aortic segments (b). Atheromatous plaques were located in the aortic arch and around the orifices of branch arteries at 12 months of age and developed at the peripheral arterial sites with age. At 36 months of age, most of the intimal surface was covered with atheromatous plaques. PFLA was the greatest in the aortic arch (AA–P.0), decreased gradually in the thoracic aorta and increased in the proximal abdominal aorta (P.3–P.4) in any age group, whereas it was small in the middle and distal thoracic aortas at 10–12 months of age and in the middle and distal abdominal aortas in any age group. The histological findings of the aortic wall were the same as those reported previously.18 Abundant cholesterol-rich foam cells were observed at 12 months of age in the ascending, proximal thoracic and proximal abdominal aortas. The foam cells were being replaced by proliferated collagenous and elastin fibres with age.

Photographs of the intimal surface of the atherosclerotic aorta (a) and age-related change in percent fractional lesioned area (PFLA) (b) in different aortic segments in the KHC rabbits. The data are presented as mean±s.d. *P<0.05, **P<0.01, ***P<0.001, d: KHC 10–12 months (M) vs. KHC 22–24 months, e: KHC 10–12 months vs. KHC 34–36 months, f: KHC 22–24 months vs. KHC 34–36 months.
Age-related changes in blood pressure at different aortic positions
Systolic and diastolic blood pressures (SBPs and DBPs, respectively) at each aortic position in the normal and KHC rabbit groups were listed in Table 2. SBP was significantly greater in the KHC rabbit group than in the age-matched control group at any aortic position at different ages and increased significantly with age between AA and P.4 in the KHC rabbit group. DBP was significantly greater in the KHC rabbit group than in the age-matched control group at any aortic position, except AA, P.0, P.1, P.5 and P.6 at 34–36 months of age. MAP, PP and heart rate in the normal and KHC rabbit groups were shown in Table 3. MAP in the KHC rabbit group showed a significant increase compared with that in the age-matched control group at any aortic position, but did not increase significantly with age. PP was significantly higher in the KHC rabbit group than in the age-matched control group at AA, P.0 and P.1 at 22–24 months of age and at any aortic position at 34–36 months of age and showed age-associated increase at any aortic position. There was no significant difference in heart rate between the KHC and age-matched control rabbit groups and among the three age groups in the two strains.
Age-related changes in LPWV in different aortic segments
Figure 2 shows age-related changes in LPWV in different aortic segments in the normal and KHC rabbit groups. In the normal rabbit group, LPWV was the lowest in AA–P.0, increased slightly in the thoracic aorta and increased gradually in the abdominal aorta with increasing distance from the heart at different ages. There was no age-related significant difference in LPWV at any aortic segment. In the KHC rabbit group, LPWV was the greatest in the aortic arch, decreased gradually in the thoracic aorta and increased again in the abdominal aorta at any age. LPWV was significantly greater in the KHC rabbit group than in the age-matched control group between AA–P.0 and P.3–P.4. It is interesting that LPWV in the KHC rabbit group was almost identical to that in the age-matched control group in almost all lesion-free aortic segments. LPWV increased significantly with age in the KHC rabbit group in all of the aortic segment except P.5–P.6. The change pattern of the LPWV resembled that in the PFLA in the aortic regions proximal to P.3–P.4 in any age group.

Local pulse wave velocity (LPWV) in different aortic segments in the normal and KHC rabbits aged 10–12, 22–24 and 34–36 months. The data are presented as mean±s.d. *P<0.05, **P<0.01, ***P<0.001, a: normal 10–12 months vs. KHC 10–12 months, b: normal 22–24 months vs. KHC 22–24 months, c: normal 34–36 months vs. KHC 34–36 months, d: KHC 10–12 months vs. KHC 22–24 months, e: KHC 10–12 months vs. KHC 34–36 months, f: KHC 22–24 months vs. KHC 34–36 months.
Age-related changes in the rheological properties of the aorta
Figure 3 shows the effect of age on PE (panel a), h (panel b), D (panel c) and PEh/D (the inside value of the root sign in the Moens–Korteweg equation22, 23) (panel d) in the proximal thoracic aorta in the normal and KHC rabbit groups. The PE value was significantly greater in the KHC rabbit group than in the age-matched control group, whereas Ep at 10–12 months of age in the KHC rabbit group was nearly equal to that in the age-matched control group. The Ep value increased significantly with age in the KHC rabbit group. The h value was significantly greater in the KHC rabbit group than in the age-matched control group at 22–24 and 34–36 months of age and increased significantly with age in the KHC rabbit group. There were neither significant differences in the D value between the two groups nor significant age-related changes in the D value in the two groups. The Eph/D value was significantly greater in the KHC rabbit group than in the age-matched control group at 22–24 and 34–36 months of age and showed a significant age-related increase in the KHC rabbit group.

Pressure–strain elastic modulus of the aortic wall (a), thickness of the aortic wall (b), internal diameter of the aorta (c) and inside value of the root sign of the Moens–Korteweg equation (d) in the proximal thoracic aorta in the normal and KHC rabbits aged 10–12, 22–24 and 34–36 months. The data are presented as mean±s.d. PE: pressure–strain elastic modulus of the aortic wall, h: thickness of the aortic wall, d: internal diameter, PEh/D: inside value of the root sign of the Moens–Korteweg equation, *P<0.05, **P<0.01, ***P<0.001.
Figure 4 illustrates the effect of age on Ep (panel a), h (panel b), D (panel c) and Eph/D (panel d) in the proximal abdominal aorta in the normal and KHC rabbit groups. The Ep value showed a significant increase in the KHC rabbit group compared with that in the age-matched control group at 22–24 and 34–36 months of age and also showed a significant age-related increase in the KHC rabbit group. The h value was significantly greater in the KHC rabbit group than in the age-matched control group and increased significantly with age in the KHC rabbit group. The D value did not show any significant differences between the KHC and age-matched control rabbit groups nor any significant age-related changes in the two groups. The Eph/D value showed a significant increase in the KHC rabbit group compared with that in the age-matched control group at 22–24 and 34–36 months of age and also showed a significant age-related increase in the KHC rabbit group.

Pressure–strain elastic modulus of the circumferential aortic wall (a), thickness of the wall (b), internal diameter of the aorta (c) and inside value of the root sign of the Moens–Korteweg equation (d) in the proximal abdominal aorta in the normal and KHC rabbits aged 10–12, 22–24 and 34–36 months. See the legend of Figure 3.
Figure 5 shows the effect of age on Ep (panel a), h (panel b), D (panel c) and Eph/D (panel d) in the distal abdominal aorta (P.6) in the normal and KHC rabbit groups. There were no significant difference in Ep, h, D and Eph/D values between the KHC and age-matched control groups. The Ep and D values changed little with age in the two strains. The h and Eph/D values tended to increase slightly with age in the KHC rabbit group, which was not significant.

Pressure–strain elastic modulus of the circumferential aortic wall (a), thickness of the wall (b), internal diameter of the aorta (c) and inside value of the root sign of the Moens–Korteweg equation (d) in the distal abdominal aorta in the normal and KHC rabbits aged 10–12, 22–24 and 34–36 months. See the legend of Figure 3.
Discussion
Blood pressure level in KHC rabbits
SBP, DBP and MAP were significantly greater in the KHC rabbit group than in the age-matched control rabbit group. SBP showed the age-associated increase in the KHC rabbit group. Akita et al.24 previously measured SBP, DBP and MAP for 24 h using a telemetry system in the normal and KHC rabbits aged 5 and 10 months through a catheter chronically indwelt in the abdominal aorta under conscious conditions. They reported that SBP and DBP in the two rabbit strains were distributed below 100 and 70 mm Hg, respectively, in both light and dark phases. We recorded pulse waves under anesthetized conditions. Pentobarbital anesthesia has been shown to exert on cardiovascular system due mainly to modulating sympathetic tone.25, 26 We considered that pentobarbital sodium affected cardiovascular system and elevated strongly blood pressure level especially in the aged KHC rabbits, although precise pressor mechanism has not been investigated in the present study.
Effects of the rheological characteristics on LPWV
PWV could be theoretically expressed by the Moens–Korteweg equation: PWV=K , where K, E, h, ρ, and D are a constant, elastic modulus, wall thickness, density of blood and internal diameter, respectively.22, 23 In the present study, the Ep value at 22–24 and 34–36 months of age in the KHC rabbits showed a significant increase compared with that in the age-matched control groups in the proximal thoracic and proximal abdominal aortas and increased significantly with age in the KHC rabbit group. The h value was also significantly greater in the KHC rabbit group than in the age-matched control group in the proximal thoracic and proximal abdominal aortas and increased significantly with age in the KHC rabbit group. There was no significant difference in the D value between the normal and KHC rabbits in any age group. Although the ρ value was not determined in the present study, Hasegawa et al.27 confirmed no significant difference in the ρ value between normal and heritable hyperlipidemic rabbits. Therefore, the significant increase in LPWV at 22–24 and 34–36 months of age in the KHC rabbits is mainly due to the significant increase in the Eph/D value in the proximal thoracic and proximal abdominal aortas. The age-associated increase in LPWV in the KHC rabbit group is also mainly ascribed to the significant age-related increase in Ep and h in the proximal thoracic and proximal abdominal aortas.
, where K, E, h, ρ, and D are a constant, elastic modulus, wall thickness, density of blood and internal diameter, respectively.22, 23 In the present study, the Ep value at 22–24 and 34–36 months of age in the KHC rabbits showed a significant increase compared with that in the age-matched control groups in the proximal thoracic and proximal abdominal aortas and increased significantly with age in the KHC rabbit group. The h value was also significantly greater in the KHC rabbit group than in the age-matched control group in the proximal thoracic and proximal abdominal aortas and increased significantly with age in the KHC rabbit group. There was no significant difference in the D value between the normal and KHC rabbits in any age group. Although the ρ value was not determined in the present study, Hasegawa et al.27 confirmed no significant difference in the ρ value between normal and heritable hyperlipidemic rabbits. Therefore, the significant increase in LPWV at 22–24 and 34–36 months of age in the KHC rabbits is mainly due to the significant increase in the Eph/D value in the proximal thoracic and proximal abdominal aortas. The age-associated increase in LPWV in the KHC rabbit group is also mainly ascribed to the significant age-related increase in Ep and h in the proximal thoracic and proximal abdominal aortas.
In the relatively early-to-middle stages of atherosclerosis, the aortic wall was thickened with abundant foam cells in KHC rabbits at 10–12 months of age. The abundant foam cells are thought to endow softness to the wall,18, 28 which was thought to be partly reflected by the absence of a significant difference in Ep and LPWV in the thoracic aorta between the young-adult KHC and age-matched control rabbit groups. Farrar et al.10 reported that PWV tended to decrease at the early stage of dietary-induced atherosclerosis in cynomolgus monkeys.
LPWV increased gradually along the aorta and reached maximum in the distal abdominal aortic segment (P.5–P.6) in the normal rabbit group at any age. The Ep value increased, whereas the h and D values decreased with increasing distance from the heart. The Ep value at P.6 was nearly twice as large as that at P.1. The Eph/D value resulted in increasing toward peripheral aortic position (Figures 3, 4, 5), which was considered to be responsible for the maximum level of LPWV in P.5–P.6 in the normal rabbit group.
Change pattern of LPWV did not reflect that of PFLA in the aortic segments distal to P.3-P.4, in which PFLA decreased drastically in any age group. LPWV was the greatest in P.5–P.6 compared with that in the lesion-rich aortic segments (AA–P.0 and P.3–P.4) in the 10–12-month-old KHC rabbit group although sclerotic lesion was few in P.5–P.6. The Ep value at P.6 was nearly twice as large as that at P.1, whereas the h and D values decreased toward peripheral aortic region. The Eph/D value at P.6 resulted in exceeding that at P.1 and P.4, which was thought to be responsible mainly for reaching a maximum LPWV level in P.5–P.6 in young KHC rabbit group. LPWV reduced in the segment of P.5–P.6 in the aged KHC rabbit group. This was thought to be responsible for the decreased Ep, h, D and Eph/D values at P.6 compared with those at P.1 and P.4. LPWV in the segment of P.5–P.6 also showed no significant differences between the KHC and age-matched control rabbit groups. This was due mainly to the fact that there was no significant difference in the Ep, h, D and Eph/D values at P.6 between the KHC and age-matched control rabbit groups although the h and Eph/D values tended to increase a little in the aged KHC rabbit group.
In human studies, Zureik et al.14 observed that a significant correlation was not present between cerotid–femoral PWV and intima-media thickening after adjusting for age and blood pressure. Nishi et al.15 demonstrated no association between brachial–ankle PWV and intima-media thickening even in the presence of atheromatous plaques. Cecelja and Chowienczyk16 reported in their review that hypertension was the only risk factor of cardiovascular disease associated with the progression of cerotid–femoral PWV. Although cerotid–femoral PWV and brachial–ankle PWV are not adequate to estimate the localization of atherosclerotic lesions, LPWV makes it possible to identify the relatively early-to-middle stages of atherosclerotic lesions.
Effects of blood pressure on LPWV
PWV has been shown to be dependent on SBP3, 6, 29, 30 and DBP.6, 29, 31 Hayashi et al.32 reported that PWV from the aortic root to the bifurcation of the common iliac arteries increased by 0.54 m s−1 and 0.66 m s−1 in the young-adult normal and KHC rabbit groups, respectively, when the MAP level was increased by 20 mm Hg. In the present study, SBP, DBP, MAP (Tables 2 and 3) and LPWV (Figure 2) distributed in a relatively narrow range at different positions in the two strains. There was no significant correlation between SBP and LPWV, between DBP and LPWV and between MAP and LPWV at most aortic positions in the two rabbit strains except P.0, P.1 and P.2 in the normal rabbit group aged 34–36 months. Significant correlation may be incidentally detected depending on variation of the correlation plot within a small pressure range. SBP, DBP and MAP showed a relatively small but significant difference between the two rabbit strains at different aortic positions in any age group, which might slightly contribute to the increase in LPWV in the KHC rabbit group.
Usefulness of LPWV as an index of arterial stiffness
Augmentation index (AI) of central pressure waves has been used as an indirect index of arterial stiffness.4 AI was calculated as a ratio of the height of the early-to-late (=pulse pressure) systolic waves.33, 34 The former is mainly affected by the distensibility of the arterial wall, stroke volume or ejection rate from the left ventricle, and the latter is mainly affected by the magnitude and arrival time of reflected waves from the peripheral arterial sites.2 We reported previously that AI in the AA did not show an age-associated increase in KHC rabbits although atherosclerotic lesions were prominent in the AA and progressed with age.35 This was mainly because the height of the early as well as the late systolic waves increased progressively with age in the KHC rabbits.35 Furthermore, the rise in AI was inhibited by the increase in the early systolic pressure with the considerable increase in LPWV in the AA (Figure 2). The incremental elastic modulus of the aortic wall increased progressively with age,18 whereas stroke volume and heart rate did not show a significant age-associated change.35 The age-related decrease in the distensibility of the aortic wall does not increase AI but increases LPWV. Therefore, LPWV, rather than AI, is useful for evaluating the increase in arterial rigidity in a restricted aortic region.
Limitations
Atheromatous plaques are the most dominant in the aortic arch and around the bifurcations of branch arteries in rabbits, whereas they are prominent in the abdominal aorta in humans.12 It is necessary to consider the differences in the localization and development of atherosclerotic lesions between rabbits and humans. In this study, we measured LPWV invasively by using a catheter with multiple micromanometers at the tip in anesthetized hypercholesterolemic rabbits. However, this method is allowed in patients only during cardiac catheterization. It is therefore necessary to develop non-invasive techniques to precisely measure pulse waves and other hemodynamic parameters such as aortic diameter and wall thickness of narrowed aortic areas for LPWV measurement.
Conclusions
In conclusion, LPWV accurately detected the presence of atherosclerotic lesions and alteration in the rheological properties of the aortic wall of the aortic regions through which pulse waves travelled. LPWV could thus be a useful aid for the diagnosis of the location and severity of atherosclerotic lesions.
References
Laurent S, Cockcroft J, Van Bortel L, Boutouyrie P, Giannattasio C, Hayoz D, Pannier B, Vlachopoulos C, Wilkinson I, Struijker-Boudier H . Expert consensus document on arterial stiffness: methodological issues and clinical applications. Eur Heart J 2006; 27: 2588–2605.
O'Rourke MF, Hashimoto J . Mechanical factors in arterial aging. J Am Coll Cardiol 2007; 50: 1–13.
Avolio AP, Deng FQ, Li WQ, Luo YF, Huang ZD, Xing LF, O'Rourke MF . Effects of aging on arterial distensibility in populations with high and low prevalence of hypertension: comparison between urban and rural communities in China. Circulation 1985; 71: 202–210.
McEniery CM, Yasmin, Hall IR, Qasem A, Wilkinson IB, Cockcroft JR, on behalf of the ACCT Investigators. Normal vascular aging: differential effects on wave reflection and aortic pulse wave velocity. the Anglo-Cardiff Collaborative Trial (ACCT). J Am Coll Cardiol 2005; 46: 1753–1760.
Safar ME . Arterial aging—hemodynamic changes and therapeutic options. Nat Rev Cardiol 2010; 7: 442–449.
Yamashina A, Tomiyama H, Arai T, Koji Y, Yambe M, Motobe H, Gluniza Z, Yamamoto Y, Hori S . Nomogram of the relation of brachial-ankle pulse wave velocity with blood pressure. Hypertens Res 2003; 26: 801–806.
Blacher J, Asmar R, Djane S, London GM, Safar ME . Aortic pulse wave velocity as a marker of cardiovascular risk in hypertensive patients. Hypertension 1999; 33: 1111–1117.
Boutouyrie P, Tropeano AI, Asmar R, Gautier I, Benetos A, Lacolley P, Laurent S . Aortic stiffness is an independent predictor of primary coronary events in hypertensive patients. A longitudinal study. Hypertension 2002; 39: 10–15.
Farrar DJ, Green HP, Bond MG, Wagner WP, Gobbee RA . Aortic pulse wave velocity, elasticity and composition in a non-human primate model of atherosclerosis. Circ Res 1978; 43: 52–62.
Farrar DJ, Bond MG, Riley WA, Sawyer JK . Anatomic correlates of aortic pulse wave velocity and carotid artery elasticity during atherosclerosis progression and regression in monkeys. Circulation 1991; 83: 1754–1763.
Kurosawa T, Kusanagi M, Yamasaki Y, Senga Y, Yamamoto T . New mutant rabbit strain with hypercholesterolemia and atherosclerotic lesions produced by serial inbreeding. Lab Anim Sci 1995; 45: 385–392.
Stehbens WE . Atherosclerosis. In: Thomas CC, Stehbens WE (eds). Hemodynamics and the Blood Vessel Wall. Charles C Thomas: Illinois, USA. 1979 pp 316–374.
Sawabe M, Takahashi R, Matsushita S, Ozawa T, Arai T, Hamamatsu A, Nakahara K, Chida K, Yamanouchi H, Murayama S, Tanaka N . Aortic pulse wave velocity and the degree of atherosclerosis in the elderly: a pathological study based on 304 autopsy cases. Atherosclerosis 2005; 179: 345–351.
Zureik M, Temmar M, Adamopoulos C, Bureau JM, Courbon D, Thomas F, Bean K, Touboul PJ, Ducimetière P, Benetos A . Carotid plaques, but not common carotid intima-media thickness, are independently associated with aortic stiffness. J Hypertens 2002; 20: 85–93.
Nishi Y, Koshiyama H, Honjo S, Seino Y . Poor correlation of pulse-wave velocity and intima-media thickness in diabetic subjects. Diabetes Care 2004; 27: 2084 (abstract).
Cecelja M, Chowienczyk P . Dissociation of aortic pulse wave velocity with risk factors for cardiovascular disease other than hypertension: a systematic review. Hypertension 2009; 54: 1328–1336.
Katsuda S, Miyashita H, Hasegawa M, Machida N, Kusanagi M, Yamasaki M, Waki H, Hazama A . Characteristic change in local pulse wave velocity in different segments of the atherosclerotic aorta in KHC rabbits. Am J Hypertens 2004; 17: 181–187.
Katsuda S, Machida N, Hasegawa M, Miyashita H, Kusanagi M, Tsubone H, Hazama A . Change in the static rheological properties of the aorta in Kurosawa and Kusanagi-hypercholesterolemic (KHC) rabbits with progress of atherosclerosis. Physiol Meas 2004; 25: 505–522.
Katsuda S, Suzuki K, Koyama N, Takahashi M, Miyake M, Hazama A, Takazawa K . Safflower seed polyphenols (N-(p-coumaroyl)serotonin and N-feruloylserotonin) ameliorate atherosclerosis and distensibility of the aortic wall in Kurosawa and Kusanagi-hypercholesterolemic (KHC) rabbits. Hypertens Res 2009; 32: 944–949.
Peterson LH, Jensen RE, Parnell J . Mechanical properties of arteries in vivo. Circ Res 1960; 8: 622–639.
McDonald DA . Blood Flow in Arteries 1st edn Edward Arnold: London, UK. 1960 pp 161.
Möens AI . Die Pulskurve. E. J. Brill: Leiden, The Netherlands. 1878 pp 90.
Korteweg DJ . Über die Fortpflanzungsgeschwindigkeit des Schalles in elastischen Rohren. Ann Phys Chem Neue Folge 1878; 5: 525–542.
Akita M, Ishii K, Kuwahara M, Tsubone H . The daily pattern of cardiovascular parameters in Kurosawa and kusanagi-Hypercholesterolemic (KHC) rabbits. Exp Anim 2002; 51: 353–360.
Duan VF, Winters RW, McVabe PM, Green EJ, Schneiderman N . Basal and reactive plasma catecholamine levels under stress and anesthesia in rabbits. Physiol Behav 1994; 56: 577–583.
Teranishi Y, Iriuchijima J . Sympathetic vasoconstrictor tone induced by pentobarbital anesthesia in hindquarters of rats. Jpn J Physiol 1992; 42: 171–178.
Hasegawa M, Dobashi T, Takei S, Sakanishi A, Watanabe Y, Ito T, Shiomi M . Ultrasonic velocity measurement of the compressibility of plasma and red blood cells in normal and hyperlipidemic (WHHL) rabbits. Rep Prog Polym Phys Jpn 1988; 31: 733–736.
Newman DL, Gosling RG, Bowden NLR . Changes in aortic distensibility and area ratio with the development of atherosclerosis. Atherosclerosis 1971; 14: 231–240.
Yasmin, Brown MJ . Similarities and differences between augmentation index and pulse wave velocity in the assessment of arterial stiffness. QJM 1999; 92: 595–600.
Kim EJ, Park CG, Park JS, Suh SY, Choi CU, Kim JW, Kim SH, Lim HE, Rha SW, Seo HS, Oh DJ . Relationship between blood pressure parameters and pulse wave velocity in normotensive and hypertensive subjects: invasive study. J Hum Hypertens 2007; 21: 141–148.
Nürnberger J, Dammer S, Saez AO, Philipp T, Schäfers RF . Diastolic blood pressure is an important determinant of augmentation and pulse wave velocity in young, healthy males. J Hum Hypertens 2003; 17: 153–158.
Hayashi S, Obara S, Hazama A, Murakawa M, Katsuda S . To what extent does aortic pulse wave velocity estimate early atherosclerosis in Kurosawa and Kusanagi-hypercholesterolemic rabbits? Hypertens Res 2011; 34: 559–564.
Takazawa K, Tanaka N, Takeda K, Kurosu F, Ibukiyama C . Underestimation of vasodilator effects of nitroglycerin by upper limb blood pressure. Hypertension 1995; 26: 520–523.
Takazawa K, Tanaka N, Fujita M, Matsuoka O, Saiki T, Aikawa M, Tamura S, Ibukiyama C . Assessment of vasoactive agents and vascular aging by the second derivative of photoplethysmogram waveform. Hypertension 1998; 32: 365–370.
Katsuda S, Miyake M, Kobayashi D, Hazama A, Kusanagi M, Takazawa K . Does augmentation index of pulse waves truly increase with progression of atherosclerosis? An experimental study in hypercholesterolemic rabbits. Am J Hypertens 2013; 26: 311–317.
Acknowledgements
We thank Professor Hitoshi Yokoyama, Dr Hirono Satokawa and Dr Shinya Takase from the Department of Cardiovascular Surgery, Fukushima Medical University School of Medicine, for kindly offering us the IVUS system. We express our appreciation to Mr Haruyuki Wago for his kind technical support. We also express our gratitude to Japan Laboratory Animals for kindly offering KHC rabbits.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Katsuda, Si., Takazawa, K., Miyake, M. et al. Local pulse wave velocity directly reflects increased arterial stiffness in a restricted aortic region with progression of atherosclerotic lesions. Hypertens Res 37, 892–900 (2014). https://doi.org/10.1038/hr.2014.96
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2014.96
Keywords
This article is cited by
-
Response to Aboyans, et al.: Estimation of pulse wave velocity in patients with peripheral artery disease: a word of caution
Hypertension Research (2016)
-
Influence of the central-to-peripheral arterial stiffness gradient on the timing and amplitude of wave reflections
Hypertension Research (2016)
-
Seeking a blood pressure-independent measure of vascular properties
Hypertension Research (2016)
