
Abstract
Recent studies have suggested that not only mean blood pressure but also variability in blood pressure might be related to cardiovascular disease. The aim of this study was to investigate the association between home blood pressure variability on one occasion and markers of arterial stiffness in patients with type 2 diabetes. We investigated the relationship between the s.d. of clinic- or home-measured systolic blood pressure on one occasion and pulse wave velocity (PWV) in 332 patients with type 2 diabetes, and we evaluated whether the SD of clinic- or home-measured systolic blood pressure on one occasion was an independent determinant of PWV by multivariate linear regression analysis, after adjustment for known risk factors for arterial stiffness, including sex, age, duration of diabetes, body mass index, hemoglobin A1c, serum total cholesterol, triglycerides, smoking status, drinking alcohol, presence of antihypertensive medication, average systolic blood pressure and heart rate. Age, average morning home-measured systolic blood pressure, heart rate and PWV (r=0.259, P<0.0001) were positively correlated with the s.d. of morning home blood pressure on one occasion. Multiple regression analysis demonstrated that age, average morning home-measured systolic blood pressure (P=0.0019), heart rate and the s.d. of morning home-measured systolic blood pressure on one occasion (P=0.0159) were independently associated with PWV. In conclusion, home blood pressure variability on one occasion was correlated with PWV, independent of other known risk factors, in Japanese patients with type 2 diabetes.
Similar content being viewed by others

Introduction
The purpose of long-term care for diabetic patients is to prevent the development of diabetic complications. It is important to control blood pressure, as well as to control blood glucose, for the prevention of microvascular and macrovascular complications. Home-measured blood pressure has been found to have a stronger relationship with target organ damage than clinic-measured blood pressure in several population-based studies and prospective clinical studies.1, 2 Therefore, the utility of home blood pressure measurement has been widely accepted, and the self-measurement of home blood pressure has been widely performed in clinical practice for patients at high risk for cardiovascular disease (CVD).
The Japanese Society of Hypertension guidelines recommend only one home blood pressure measurement on one occasion,3 and the European Society of Hypertension guidelines recommend two consecutive home blood pressure measurements on one occasion.4 The American Heart Association guidelines recommend two to three consecutive home blood pressure measurements on one occasion.5 However, the clinical significance of three consecutive home blood pressure measurements has not yet been well defined.
Recent studies have suggested that not only mean home blood pressure but also day-to-day variability in home blood pressure measurements could be a simple method of providing useful clinical information for assessing cardiovascular risk.6, 7 It is evident that blood pressure variations assessed over different time periods can reflect the impact of different physiological factors.8 Increased short-term blood pressure variability, including blood pressure variability on one occasion, results from a depressed baroreflex function, which is potentially associated with increased stiffness of the large arteries.9 Changes in respiration and rhythmic alterations in the central autonomic drive, mediated by baroreflex mechanisms, are important determinants of short-term blood pressure variability, including blood pressure variability on one occasion.10 We hypothesized that home-measured blood pressure variability on one occasion, as one measurement of short-term blood pressure variability and calculated using three consecutive measurements, would be correlated with arterial stiffness.
Arterial stiffness can be assessed simply, noninvasively and reproducibly by measuring pulse wave velocity (PWV) along the thoracoabdominal aorta.11 PWV is a marker for both the severity of vascular damage and prognosis in atherosclerotic vascular disease.12, 13 Therefore, we evaluated the relationship between the variability of clinic-measured and morning or evening home-measured systolic blood pressure on one occasion, calculated by three consecutive measurements, and a marker of arterial stiffness evaluated by PWV in patients with type 2 diabetes. Furthermore, we also investigated the association between day-to-day home-measured blood pressure variability and PWV in this study, and we evaluated which was more closely associated with PWV: home-measured blood pressure variability on one occasion or day-to-day home-measured blood pressure variability.
Methods
Patients
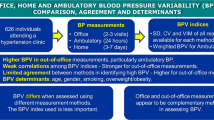
Home-measured blood pressure measurements were obtained in patients with type 2 diabetes who had regularly attended the diabetes outpatient clinic at the Hospital of Kyoto Prefectural University of Medicine and at four other general hospitals, as previously reported.14 A total of 954 patients with type 2 diabetes agreed to participate in this study. First, 31 patients were excluded who conducted home blood pressure measurements for fewer than four consecutive days.15 We randomly measured PWV, and 567 patients were also excluded whose data for PWV were not available because of the limited capacity to perform PWV at every hospital. In addition, 10 patients who had advanced renal dysfunction (serum creatinine ⩾2.0 mg dl−1) and 14 patients whose ABI (ankle-brachial index) was <0.9516 were excluded from the analyses. Finally, 332 patients comprised the study population (175 men, 157 women), including 74 at Kyoto Prefectural University of Medicine, 109 at Kyoto First Red Cross Hospital, 6 at Kyoto Second Red Cross Hospital, 138 at Osaka General Hospital of West Japan Railway Company and 5 at Social insurance Kyoto Hospital.
Type 2 diabetes was diagnosed according to the Report of the Expert Committee on the Diagnosis and Classification of Diabetes Mellitus.17 Retinopathy was assessed with the patient in a state of mydriasis by ophthalmologists who were unaware of the data, and retinopathy was graded as follows: no diabetic retinopathy; simple diabetic retinopathy; and proliferative, including preproliferative, diabetic retinopathy. If the findings in the left and right fundi were discordant, the worse side was taken as representative for the subject.
Nephropathy was graded as follows: normoalbuminuria, urinary albumin excretion <30 mg per gram of creatinine (mg g−1 Cr); microalbuminuria, 30–300 mg g−1 Cr; or macroalbuminuria, more than 300 mg g−1 Cr. Neuropathy was defined by the diagnostic criteria for diabetic neuropathy proposed by the Diagnostic Neuropathy Study Group.18 In brief, in the absence of peripheral neuropathies, diabetic neuropathy was diagnosed based on two or more of the following: neuropathic symptoms, such as numbness, paresthesia and neuropathic pain; decreased or absent ankle reflex (bilateral); and decreased distal sensation. CVD was defined as a previous myocardial or cerebral infarction, based on the clinical history or physical examination. Subjects were classified as nonsmokers, past smokers or current smokers, according to a self-administered questionnaire.
Study design
We designed a cross-sectional multicenter study in general hospitals located in the Kansai area in Japan. Clinic-measured blood pressure variability was defined as the s.d. of blood pressure, calculated by three consecutive measurements on one occasion, and home-measured blood pressure variability was defined as the s.d. of blood pressure, calculated by three consecutive measurements, at home every morning or evening for 14 days. Day-to-day home-measured systolic blood pressure variability was defined as the s.d. of mean morning or evening blood pressure calculated by three consecutive measurements for 14 days.
First, we investigated the relationship between the s.d. of clinic-measured and morning or evening home-measured systolic blood pressure on one occasion and PWV using linear regression analysis. Second, we compared the s.d. of clinic-measured and morning or evening home-measured systolic blood pressure on one occasion in various groups, including groups based on sex, degree of diabetic retinopathy or nephropathy, smoking status, habit of drinking alcohol, presence of diabetic neuropathy, CVD and antihypertensive medication. Third, we evaluated whether the s.d. of clinic-measured and morning or evening systolic blood pressure were independent determinants of PWV by multivariate linear regression analysis after adjustment for the following variables, which are known risk factors for arterial stiffness: sex, age, duration of diabetes, body mass index, hemoglobin A1c, total cholesterol, triglycerides, smoking status, alcohol consumption, antihypertensive medication, average systolic blood pressure and heart rate.
Finally, we investigated the relationship between the SD of morning home-measured diastolic blood pressure on one occasion or morning home-measured heart rate on one occasion and PWV. We compared the correlation between the s.d. of morning home-measured systolic blood pressure on one occasion and PWV in patients treated with and without antihypertensive medication. In addition, we investigated the relationship between the s.d. of morning home-measured systolic blood pressure at one occasion on day 1 and PWV. We compared the correlation between the s.d. of morning home-measured systolic blood pressure on one occasion and PWV when compared at 5, 7 and 14 days of morning home blood pressure measurements. Furthermore, we investigated the relationship between the s.d. of day-to-day home-measured systolic blood pressure for 14 days and PWV by linear and multiple regression analyses. This study was approved by the local research ethics committee and was conducted in accordance with the Declaration of Helsinki, and informed consent was obtained from all of the participants.
Data collection
Blood samples for biochemical measurements were obtained at the hospital. Serum total cholesterol, triglycerides and high-density lipoprotein cholesterol concentrations were assessed using standard enzymatic methods. HemoglobinA1c was assayed using high-performance liquid chromatography, with the standard provided by the National Glycohemoglobin Standardization Program. Urinary albumin excretion was measured with an immunoturbidimetric assay. A mean value for urinary albumin excretion was determined from three urine collections. Information, including age, duration of diabetes, smoking and alcohol drinking status, was obtained at the time of the clinic blood pressure measurement.
Home blood pressure measurements were self-measured using an automatic memory-equipped device (HEM-70801C; Omron Healthcare Co. Ltd, Kyoto, Japan) that uses the cuff-oscillometric method to generate a digital display of heart rate and systolic/diastolic blood pressure value. The HEM-70801C employs the identical components and blood pressure-determining algorithm to those of another device, the HEM-705IT, which was previously validated and satisfied the criteria of the British Hypertension Society protocol.19
The patients received written instructions and individual guidance on how to self-measure their blood pressure in the clinic on one occasion in triplicate and their morning and evening home blood pressure measurements on one occasion in triplicate for 14 consecutive days. Clinic blood pressure was measured using the same device as that used for home-measured blood pressure. Three consecutive measurements were obtained on the non-dominant arm at 15-s intervals after a 5-min rest in the sitting position under the observation of expert nurses. The arm circumferences of the patients ranged between 22 and 32 cm, so the standard arm cuff was able to be used for blood pressure measurements in all of the patients. The measurements of morning home blood pressure were obtained within 1 h of waking, before breakfast or taking any drugs, with the patient seated and having rested for at least 5 min.3 The measurements of evening home blood pressure were obtained in a homologous manner, just before the patient went to bed. We calculated the s.d. as an indicator of the variability of systolic blood pressure.
Measurement of PWV
Brachial-ankle PWV was measured using a Colin Waveform Analyzer (form PWV/ABI/TBI; Colin Medical Technology, Komaki, Japan), which simultaneously measures pulse volumes in the brachial and posterior tibial or toe arteries using an oscillometric method, together with bilateral arm and ankle or toe blood pressure measurement. PWV was measured after allowing the patient to rest in the supine position for at least 5 min. Details of the method have been described elsewhere.20 After bilateral determination of brachial-ankle PWV, the higher value was taken as representative for each subject.
Statistical analysis
Means and frequencies of potential confounding variables were calculated. Unpaired Student’s t-tests or one-way analysis of variance, followed by the post-hoc test with Scheffe, were conducted to assess the statistical significance of differences between groups, using Stat View software (version 5.0; SAS Institute, Cary, NC, USA). The relationships between the s.d. of clinic-measured and morning or evening home-measured systolic blood pressure on one occasion and age, glycemic control, PWV or other variables were examined by Pearson’s correlation analyses. To examine the effects of various factors on PWV, the following factors were considered simultaneously as independent variables for multiple regression analysis: sex (female=0, male=1), age, duration of diabetes, body mass index, hemoglobinA1c, serum total cholesterol, triglycerides, smoking status (none=0, past=1, current=2), alcohol consumption (none=0, social=1, everyday=2), presence of antihypertensive medication (angiotensin II receptor blocker and/or angiotensin-converting enzyme inhibitor, calcium channel blocker, diuretics, α blocker or β blocker) (no=0, yes=1), average systolic blood pressure, heart rate and s.d. as measured in the clinic, and morning or evening home-measured systolic blood pressure on one occasion. All continuous variables are presented as the mean±s.d. A P-value <0.05 was considered statistically significant.
Results
The clinical characteristics of the patients with type 2 diabetes are shown in Table 1, and the relationships between the s.d. of clinic-measured and morning or evening home-measured systolic blood pressure on one occasion and other variables are shown in Table 2. The average numbers of morning and evening home systolic blood pressure measurements per patient over the 14-day study period were 39.3±6.4 and 37.3±8.0, respectively. Average clinic-measured systolic blood pressure was positively correlated with the s.d. of clinic-measured systolic blood pressure. Age, average morning home-measured systolic blood pressure, heart rate and PWV were positively correlated with the s.d. of morning home-measured systolic blood pressure on one occasion, and age, average evening home-measured systolic blood pressure and PWV were positively correlated with the s.d. of evening home-measured systolic blood pressure on one occasion.
The s.d. of morning home-measured systolic blood pressure on one occasion was higher in patients with macroalbuminuria compared with that of patients with normoalbuminuria (Table 3). The s.d. of clinic-measured and morning or evening home-measured systolic blood pressure on one occasion were not different according to sex, degree of diabetic retinopathy, smoking or alcohol consumption, or the presence of diabetic neuropathy, CVD or antihypertensive medication. The s.d. of morning or evening home-measured systolic blood pressure on one occasion was lower in patients treated with α blockers than in patients treated without them, whereas the s.d. of evening home-measured systolic blood pressure on one occasion was higher in patients treated with β blockers than in patients treated without them.
Multiple regression analysis demonstrated that age, α blocker use, average clinic-measured systolic blood pressure and heart rate were independently associated with PWV (Table 4). Age, average morning home-measured systolic blood pressure, heart rate and the s.d. of morning home-measured systolic blood pressure on one occasion were independently associated with PWV. Age, body mass index, average evening home-measured systolic blood pressure, heart rate and the s.d. of evening home-measured systolic blood pressure on one occasion were independently associated with PWV.
The average clinic-measured and morning and evening home-measured diastolic blood pressure measurements were 78±12, 75±10 and 70±10 mm Hg, respectively, and the average clinic-measured and morning and evening home-measured heart rates were 73±11, 68±9 and 73±10 beats per min, respectively. The s.d. of morning-measured home diastolic blood pressure on one occasion was positively correlated with PWV (r=0.216, P=0.0001); however, the s.d. of morning home-measured diastolic blood pressure on one occasion was not independently associated with PWV in multiple regression analysis (β=0.109, P=0.0822). The s.d. of morning home-measured heart rate at one occasion was not correlated with PWV (r=0.033, P=0.5465). The correlation between the s.d. of morning home-measured systolic blood pressure on one occasion and PWV was similar between patients treated with (r=0.214, P=0.0056) and without antihypertensive medication (r=0.232, P=0.0030). The two regression lines in patients treated with or without antihypertensive medication were not significantly different (P=0.59 by linear regression analysis using R). In addition, the s.d. of morning home-measured systolic blood pressure on one occasion on day 1 was significantly correlated with PWV (r=0.174, P=0.0018), and the correlation between the s.d. of morning home-measured systolic blood pressure on one occasion and PWV did not differ when compared at 5 (r=0.253, P<0.0001), 7 (r=0.224, P< 0.0001) and 14 days (r=0.259, P< 0.0001) of morning home blood pressure measurements (P>0.05 by linear regression analysis using R). Furthermore, the s.d. of day-to-day morning (r=0.169, P=0.0024) or evening (r=0.177, P=0.0015) home-measured systolic blood pressure was significantly correlated with PWV. Multiple regression analysis demonstrated that age, systolic blood pressure and heart rate were independently associated with PWV (Supplementary Table S1); however, the s.d. of day-to-day home-measured systolic blood pressure was not.
Discussion
In this study, we revealed that the variability of morning or evening home-measured systolic blood pressure on one occasion was significantly correlated with PWV independent of known risk factors for arterial stiffness, including sex, age, duration of diabetes, body mass index, hemoglobin A1c, serum total cholesterol, triglycerides, smoking status, alcohol consumption, presence of antihypertensive medication, average systolic blood pressure and heart rate. To our knowledge, this is the first study indicating the positive correlation of home blood pressure variability on one occasion with PWV as a marker of arterial stiffness in patients with type 2 diabetes.
The Japanese Society of Hypertension guidelines recommend only one home blood pressure measurement on one occasion,3 because it is more convenient for subjects and results in good compliance and good equivalence for comparison.21 The European Society of Hypertension guidelines recommend two consecutive home blood pressure measurements on one occasion.4 This recommendation is based on the evidence that regression to the mean during consecutive measurements on each occasion is frequently observed after long-term monitoring.22 Moreover, the American Heart Association guidelines recommend the two to three consecutive home blood pressure measurements on one occasion.5 The optimal schedule for home blood pressure measurements should be determined by its relationship to cardiovascular risk and its ability to provide a reliable and reproducible assessment for each individual. We adopted three consecutive home blood pressure measurements on one occasion and found that home-measured blood pressure variability on one occasion was correlated with arterial stiffness. Therefore, we believe that three consecutive measurements on one occasion would also be clinically significant.
Recent studies have suggested that obtaining not only average home-measured blood pressure but also the day-to-day variability in home-measured blood pressure could be a simple method of providing useful clinical information for assessing cardiovascular risk.6, 7 To our surprise, however, the s.d. of day-to-day home-measured systolic blood pressure was not associated with PWV in multiple regression analysis. Home-measured blood pressure variability on one occasion was more strongly associated with arterial stiffness than was the s.d. of day-to-day home-measured systolic blood pressure.
Increased short-term blood pressure variability, including home-measured blood pressure variability on one occasion, results from a depressed baroreflex function, which is potentially associated with increased stiffness of the large arteries.9 Changes in respiration and rhythmic alterations in central autonomic drive, mediated by baroreflex mechanisms, are important determinants of short-term blood pressure variability, including blood pressure variability on one occasion.10
The adverse effects of increased blood pressure variability are possibly related to the greater traumatic effects of wider blood pressure swings on the vessel walls, promoting early target organ damage.
Age, average systolic blood pressure and heart rate, which are risk factors for increased stiffness of the large arteries, were correlated in the present study with the s.d. of morning home-measured systolic blood pressure on one occasion. Recent reports have identified the factors associated with day-to-day variability in self-measured home blood pressure.23, 24 Variations in the patient’s activities, underlying diseases such as hypertension and diabetes mellitus, and poor drug compliance also affect the day-to-day variability of home-measured systolic blood pressure.
We cannot explain the reason that the s.d. of morning or evening home-measured systolic blood pressure on one occasion was lower in patients treated with α blockers than in patients treated without them, whereas the s.d. of evening home-measured systolic blood pressure on one occasion was higher in patients treated with β blockers than in patients treated without them. Possible explanations for these results are that α blockers reduce autonomic nervous system activation, which is one of the causes of greater variation between measurements. As for β blockers, changes in peripheral vascular resistance are perhaps the most likely explanation: β blockers reduce arterial compliance by vasoconstriction. Moreover, Cahan et al.25 reported that lower heart rate was associated with increased blood pressure variability during ambulatory blood pressure monitoring, although their results were statistically significant because the number of patients treated with α blockers or β blockers was too small. Therefore, further studies would be needed to clarify these observations.
It is known that antihypertensive medications can delay the development of albuminuria or atherosclerosis in patients with diabetes.26 Variability in systolic blood pressure can be affected by antihypertensive medications, including angiotensin-converting enzyme inhibitors, angiotensin II receptor blockers and β blockers.27 However, in our study, variability in morning or evening home-measured systolic blood pressure on one occasion was independently associated with PWV, even after adjustment for antihypertensive medications (angiotensin II receptor blockers and/or angiotensin-converting enzyme inhibitors, calcium channel blockers, diuretics, α blockers or β blockers).
The magnitude of correlation between the s.d. of morning or evening home-measured systolic blood pressure on one occasion and PWV was less than that between the average clinic-measured and morning or evening home-measured systolic blood pressure and PWV. However, the s.d. of morning or evening home-measured systolic blood pressure on one occasion was associated with PWV, even after adjustment for average morning or evening home-measured blood pressure. This finding indicates that both the variability of home-measured systolic blood pressure on one occasion and average home-measured systolic blood pressure are independently associated with arterial stiffness. The reasons for the relationship between home-measured blood pressure variability on one occasion and PWV and the lack of a relationship between the variability in clinic-measured systolic blood pressure on one occasion and PWV were not clearly determined by this study. Home blood pressure measurement has been reported to be more reliable than clinic measurement, because it offers better reproducibility.28 In addition, home blood pressure measurement has been more strongly associated with target organ damage and with offering better prognostic value than clinic-measured blood pressure in predicting mortality or cardiovascular events.1, 2 Taken together, the s.d. of morning or evening home-measured systolic blood pressure could be a simple method of providing useful clinical information for assessing arterial stiffness in addition to known risk factors, including clinic-measured and morning or evening home-measured systolic blood pressure.
This study has some limitations that require consideration. First, the correlation between home-measured blood pressure variability on one occasion and PWV was weak, although it was statistically significant. Second, poor patient compliance with antihypertensive medication might have had a role in increasing blood pressure variability via inadequate blood pressure control in medical practice. However, the results were similar after patients taking antihypertensive medication were excluded. Therefore, poorer compliance with medication alone might not fully explain the larger variability in blood pressure. Third, the patients measured their blood pressure under relatively controlled conditions and received individual guidance on how to perform the measurements correctly. However, it is still possible that the measurement procedure could have affected blood pressure variability. Fourth, although the latest home blood pressure guideline29 recommends a 1-min interval between readings, in the present study, we set the interval at 15 s30 to improve the patients’ compliance with home blood pressure measurements. Fifth, the patients self-measured clinic blood pressure on one occasion in triplicate and morning and evening home blood pressure on one occasion in triplicate for 14 consecutive days. Therefore, the s.d. of clinic-measured systolic blood pressure was higher than that of morning systolic blood pressure. However, the s.d. of morning home-measured systolic blood pressure on one occasion on day 1 was also significantly correlated with PWV. Sixth, it is not clear whether the correlation between the s.d. of clinic-measured systolic blood pressure on one occasion and PWV in this study is applicable to generally measured clinic blood pressure because we used self-measured clinic blood pressure in this study. Finally, the cause-effect relationship between home-measured blood pressure variability on one occasion and PWV was not clearly determined, because this study was cross-sectional. However, it was reported that in sinoaortic-denervated rats (an experimental model of high variability of blood pressure without hypertension), variability in blood pressure was a more critical determinant than blood pressure level for cardiac damage, renal lesions and aortic hypertrophy.31 Moreover, a reduction in blood pressure variability, resulting from various antihypertensive regimens in spontaneously hypertensive rats, was shown to contribute significantly and independently to organ protection.32, 33
In general, we gave little attention to whether home blood pressure variability on one occasion was associated with arterial stiffness. In this context, it might be presumed that home blood pressure variability on one occasion should be taken into consideration in the treatment of patients with type 2 diabetes. In the future, we must investigate what the optimal range is for the s.d. of morning home-measured systolic blood pressure on one occasion, how to use this measurement, how to reduce it and whether such a reduction will improve prognosis.
Conclusions
Home blood pressure variability on one occasion was associated with PWV, independent of other known risk factors for arterial stiffness, in Japanese patients with type 2 diabetes. Large, prospective studies are needed to confirm the variability in morning home-measured systolic blood pressure on one occasion as an associated risk factor for arterial stiffness in patients with type 2 diabetes.
References
Ohkubo T, Imai Y, Tsuji I, Nagai K, Kato J, Kikuchi N, Nishiyama A, Aihara A, Sekino M, Kikuya M, Ito S, Satoh H, Hisamichi S . Home blood pressure measurement has a stronger predictive power for mortality than does screening blood pressure measurement: a population-based observation in Ohasama, Japan. J Hypertens 1998; 16: 971–975.
Sega R, Trocino G, Lanzarotti A, Carugo S, Cesana G, Schiavina R, Valagussa F, Bombelli M, Giannattasio C, Zanchetti A, Mancia G . Alterations of cardiac structure in patients with isolated office, ambulatory, or home hypertension: data from the general population (Pressione Arteriose Monitorate E Loro Associazioni [PAMELA]Study). Circulation 2001; 104: 1385–1392.
Imai Y, Otsuka K, Kawano Y, Shimada K, Hayashi H, Tochikubo O, Miyakawa M, Fukiyama K . Japanese Society of Hypertension: Japanese society of hypertension (JSH) guidelines for self-monitoring of blood pressure at home. Hypertens Res 2003; 26: 771–782.
Parati G, Stergiou GS, Asmar R, Bilo G, de Leeuw P, Imai Y, Kario K, Lurbe E, Manolis A, Mengden T, O'Brien E, Ohkubo T, Padfield P, Palatini P, Pickering TG, Redon J, Revera M, Ruilope LM, Shennan A, Staessen JA, Tisler A, Waeber B, Zanchetti A, Mancia G, ESH Working Group on Blood Pressure Monitoring. European Society of Hypertension practice guidelines for home blood pressure monitoring. J Hum Hypertens 2010; 24: 779–785.
Pickering TG, Miller NH, Ogedegbe G, Krakoff LR, Artinian NT, Goff D . American Heart Association; American Society of Hypertension; Preventive Cardiovascular Nurses Association: call to action on use and reimbursement for home blood pressure monitoring: executive summary: a joint scientific statement from the American Heart Association, American Society of Hypertension, and Preventive Cardiovascular Nurses Association. Hypertension 2008; 52: 10–29.
Kikuya M, Ohkubo T, Metoki H, Asayama K, Hara A, Obara T, Inoue R, Hoshi H, Hashimoto J, Totsune K, Satoh H, Imai Y . Day-by-day variability of blood pressure and heart rate at home as a novel predictor of prognosis: the Ohasama study. Hypertension 2008; 52: 1045–1050.
Johansson JK, Niiranen TJ, Puukka PJ, Jula AM . Prognostic value of the variability in home-measured blood pressure and heart rate: the Finn-Home Study. Hypertension 2012; 59: 212–218.
Parati G, Bilo G . Calcium antagonist added to angiotensin receptor blocker: a recipe for reducing blood pressure variability?: evidence from day-by-day home blood pressure monitoring. Hypertension 2012; 59: 1091–1093.
Parati G, Di Rienzo M, Mancia G . Dynamic modulation of baroreflex sensitivity in health and disease. Ann NY Acad Sci 2001; 940: 469–487.
Mancia G, Di Rienzo M, Parati G, Grassi G . Sympathetic activity, blood pressure variability and end organ damage in hypertension. J Hum Hypertens 1997; 11: S3–S8.
Asmar R, Benetos A, Topouchian J, Laurent P, Pannier B, Brisac AM, Target R, Levy BI . Assessment of arterial distensibility by automatic pulse wave velocity measurement: Validation and clinical application studies. Hypertension 1995; 26: 485–490.
Yamashina A, Tomiyama H, Arai T, Hirose K, Koji Y, Hirayama Y, Yamamoto Y, Hori S . Brachial-ankle pulse wave velocity as a marker of atherosclerosis vascular damage and cardiovascular risk. Hypertens Res 2003; 26: 615–622.
Vlachopoulos C, Aznaouridis K, Stefanadis C . Prediction of cardiovascular events and all-cause mortality with arterial stiffness: a systematic review and meta-analysis. J Am Coll Cardiol 2010; 55: 1318–1327.
Ushigome E, Fukui M, Sakabe K, Tanaka M, Inada S, Omoto A, Tanaka T, Fukuda W, Atsuta H, Ohnishi M, Mogami S, Kitagawa Y, Oda Y, Yamazaki M, Hasegawa G, Nakamura N . Uncontrolled home blood pressure in the morning is associated with nephropathy in Japanese type 2 diabetes. Heart Vessels 2011; 26: 609–615.
Johansson JK, Niiranen TJ, Puukka PJ, Jula AM . Optimal schedule for home blood pressure monitoring based on a clinical approach. J Hypertens 2010; 28: 259–264.
Motobe K, Tomiyama H, Koji Y, Yambe M, Gulinisa Z, Arai T, Ichihashi H, Nagae T, Ishimaru S, Yamashina A . Cut-off value of the ankle-brachial pressure index at which the accuracy of brachial-ankle pulse wave velocity measurement is diminished. Circ J 2005; 69: 55–60.
The Expert Committee on the Diagnosis and Classification of Diabetes Mellitus. Report of the expert committee on the diagnosis and classification of diabetes mellitus. Diabetes Care 2002; 25: S5–20.
Yasuda H, Sanada M, Kitada K, Terashima T, Kim H, Sakaue Y, Fujitani M, Kawai H, Maeda K, Kashiwagi A . Rationale and usefulness of newly devised abbreviated diagnostic criteria and staging for diabetic polyneuropathy. Diabetes Res Clin Pract 2007; 77: S178–S183.
Coleman A, Freeman P, Steel S, Shennan A . Validation of the Omron 705IT (HEM-759-E) oscillometric blood pressure monitoring device according to the British Hypertension Society protocol. Blood Press Monit 2006; 11: 27–32.
Yamashina A, Tomiyama H, Takeda K, Tsuda H, Arai T, Hirose K, Koji Y, Hori S, Yamamoto Y . Validity, reproducibility, andclinicalsignificance of noninvasive brachial-ankle pulse wave velocitymeasurement. Hypertens Res 2002; 25: 359–364.
Kawabe H, Saito I . Which measurement of home blood pressure should be used for clinical evaluation when multiple measurements are made? J Hypertens 2007; 25: 1369–1374.
Stergiou GS, Skeva II, Zourbaki AS, Mountokalakis TD . Self-monitoring of blood pressure at home: how many measurements are needed? J Hypertens 1998; 16: 725–731.
Kato T, Kikuya M, Ohkubo T, Satoh M, Hara A, Obara T, Metoki H, Asayama K, Hirose T, Inoue R, Kanno A, Totsune K, Hoshi H, Satoh H, Imai Y . Factors associated with day-by-day variability of self-measured blood pressure at home: the Ohasama study. Am J Hypertens 2010; 23: 980–986.
Johansson JK, Niiranen TJ, Puukka PJ, Jula AM . Factors affecting the variability of home-measured blood pressure and heart rate: the Finn-home study. J Hypertens 2010; 28: 1836–1845.
Cahan A, Ben-Dov IZ, Bursztyn M . Association of heart rate with blood pressure variability: implications for blood pressure measurement. Am J Hypertens 2012; 25: 313–318.
Sowers JR, Epstein M, Frohlich ED . Diabetes, hypertension, and cardiovascular disease: an update. Hypertension 2001; 37: 1053–1059.
Webb AJ, Fischer U, Mehta Z, Rothwell PM . Effects of antihypertensive-drugclass on interindividual variation in blood pressure and risk of stroke: asystematic review and meta-analysis. Lancet 2010; 375: 906–915.
Sakuma M, Imai Y, Nagai K, Watanabe N, Sakuma H, Minami N, Satoh H, Abe K . Reproducibility of home blood pressure measurements over a 1-year period. Am J Hypertens 1997; 10: 798–803.
Parati G, Stergiou GS, Asmar R, Bilo G, de Leeuw P, Imai Y, Kario K, Lurbe E, Manolis A, Mengden T, O'Brien E, Ohkubo T, Padfield P, Palatini P, Pickering T, Redon J, Revera M, Ruilope LM, Shennan A, Staessen JA, Tisler A, Waeber B, Zanchetti A, Mancia G . ESH Working Group on Blood Pressure Monitoring: European Society of Hypertension guidelines for blood pressure monitoring at home: a summary report of the Second International Consensus Conference on Home Blood Pressure Monitoring. J Hypertens 2008; 26: 1505–1526.
Yarows SA, Patel K, Brook R . Rapid oscillometric blood pressure measurement compared to conventional oscillometric measurement. Blood Press Monit 2001; 6: 145–147.
Miao CY, Xie HH, Zhan LS, Su DF . Blood pressure variability is more important than blood pressure level in determination of end-organ damage in rats. J Hypertens 2006; 24: 1125–1135.
Liu JG, Xu LP, Chu ZX, Miao CY, Su DF . Contribution of blood pressure variability to the effect of nitrendipine on end-organ damage in spontaneously hypertensive rats. J Hypertens 2003; 21: 1961–1967.
Xie HH, Miao CY, Jiang YY, Su DF . Synergism of atenolol and nitrendipine on hemodynamic amelioration and organ protection in hypertensive rats. J Hypertens 2005; 23: 193–201.
Acknowledgements
We thank Naoko Higo, Machiko Hasegawa and Terumi Kaneko of Kyoto Prefectural University of Medicine for teaching the patients how to measure their blood pressure and Sayoko Horibe, Hiroko Kawamura and Sanae Utena of Kyoto Prefectural University of Medicine for their secretarial assistance.
Author contributions
MF researched the data and wrote the manuscript, EU researched the data and contributed to the discussion, MT researched the data and contributed to the discussion, MH contributed to the discussion, TT researched the data, HA researched the data, MO researched the data, YO researched the data, GH researched the data and contributed to the discussion and NN researched the data and reviewed/edited the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Hypertension Research website
Supplementary information
Rights and permissions
About this article
Cite this article
Fukui, M., Ushigome, E., Tanaka, M. et al. Home blood pressure variability on one occasion is a novel factor associated with arterial stiffness in patients with type 2 diabetes. Hypertens Res 36, 219–225 (2013). https://doi.org/10.1038/hr.2012.177
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2012.177
Keywords
This article is cited by
-
Relationship between defecation status and blood pressure level or blood pressure variability
Hypertension Research (2024)
-
Short-term blood pressure variability as a potential therapeutic target for kidney disease
Clinical Hypertension (2023)
-
Novel Indices of Home Blood Pressure Variability and Hypertension-Mediated Organ Damage in Treated Hypertensive Patients
High Blood Pressure & Cardiovascular Prevention (2021)
-
Modulation of blood pressure-lowering effects of dark chocolate according to an insulin sensitivity-randomized crossover study
Hypertension Research (2020)
-
The Japanese Society of Hypertension Guidelines for the Management of Hypertension (JSH 2019)
Hypertension Research (2019)
