
Abstract
It is well known that blood pressure (BP) management reduces the incidence of cerebrovascular and cardiovascular events. However, it is unclear how many of these events occur in hypertensive patients who receive pharmacological treatment. The aim of this survey was to evaluate the occurrence rate of both types of events in patients receiving valsartan-based treatment. Of 30 366 patients treated with valsartan, 28 356 patients were observed for 2.93 years. Antihypertensive drugs other than valsartan were used in 56.8% of patients. After the administration of valsartan, the systolic and diastolic BP significantly decreased from 161.1±19.1/90.4±13.1 to 139.9±18.1/79.6±11.9 mm Hg. Cerebrovascular events were observed in 550 patients (1.94%, 9.29/1000 patient-years), and cardiac events were observed in 576 patients (2.03%, 9.73/1000 patient-years). A comparative analysis of the hazard ratios for cerebrovascular and cardiac events according to the BP level at the endpoint showed a BP-dependent reduction of risk for cerebrovascular events, and the change in risk exhibited a J-curve phenomenon in the relationship between cardiac events and systolic BP. The J-curve phenomenon was not observed in patients aged <75 years, but it was observed for the systolic BP in patients aged ⩾75 years. Adverse drug reactions were observed in 1925 of 28 420 patients (6.77%). This post-marketing surveillance data for valsartan showed the outcomes for treated hypertensive patients in a large population in Japan who were followed for up to 3 years. These data will add important knowledge regarding the treatment of hypertension in Japan.
Similar content being viewed by others
Introduction
The Seventh Report of the Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure advocates that the ultimate public health goal of antihypertensive therapy is the reduction of cardiovascular and renal morbidity and mortality.1 Many studies have reported the beneficial effect of antihypertensive treatment in reducing cerebrovascular and cardiovascular events.2, 3, 4 However, a substantial risk remains even for patients receiving antihypertensive treatment.
In the Japanese Society of Hypertension Guidelines for the Management of Hypertension 2009 (JSH 2009),5 patients are stratified into risk groups for cerebrovascular and cardiovascular diseases according to the severity of the hypertension and the presence/absence of major risk factors (complications and medical history). The JSH 2009 specifies that the treatment goals should be determined according to the risk stratification and recommends that patients in the high-risk group should be strictly managed.
Since 1980, the leading cause of death in Japan has been malignant neoplasm and mortality from malignant neoplasm has been steadily increasing up to the present. The number of deaths from heart diseases have slightly increased; however, there has been a trend toward decreased mortality from cerebrovascular diseases since 1970.6 These data suggest that the antihypertensive treatments given over the last 40 years may have suppressed the occurrence of cerebrovascular events, but not cardiovascular events. The JSH 2009 guideline for antihypertensive therapy clearly recommends strict blood pressure (BP) control based on a number of clinical trials. However, the percentage of patients with good BP control is not high. Mori et al.7 reported that the percentage of patients who could achieve their BP goals (<140/90 mm Hg) was 40.7% in the best control group, indicating that strict treatment of hypertension needs to be improved.
It is now well recognized that treating hypertension reduces the risk of cerebrovascular and cardiovascular events. It is also known from epidemiologic studies evaluating BP in untreated individuals that lower BP is associated with a lower risk.8 However, there are not enough reports regarding the incidence rates of cerebrovascular and cardiovascular events in patients under antihypertensive treatment in Japan. An investigation of the occurrence rates of both events is required to provide valuable insight into the cerebrovascular and cardiovascular mortality and morbidity rates in patients receiving antihypertensive treatment.
Valsartan, an angiotensin II receptor blocker, was approved for the treatment of hypertension in Japan in September 2000, and it has since been in wide clinical use.9 In Japan, pharmaceutical companies are required to conduct post-marketing surveillance to assess the safety and efficacy of drugs prescribed in clinical practice after their launch. To evaluate the occurrence of cerebrovascular and cardiac events in patients treated with antihypertensive therapy, this survey, the Japanese Survey for Valsartan In Deployment (J-VALID), was conducted in patients receiving valsartan for the treatment of hypertension as a post-marketing surveillance for valsartan in Japan.
Methods
Study design
This prospective survey with a central registry was designed as a designated drug use investigation. The patient enrollment period was 2 years, and the patient observation period was 3 years; that is, the study period was from October 2002 to September 2007. The subjects of the survey were patients who were given valsartan for the first time to treat hypertension, regardless of whether they were receiving other antihypertensive agents during the enrollment period. The patient registration form was sent to the registration center within 4 weeks of initiation of treatment with valsartan.
No interventional limits were set in the survey because post-marketing surveillance should be conducted in usual clinical practice according to Japanese regulations. The investigators who participated in this survey reported their clinical findings once per year, and the adverse events, including cerebrovascular and cardiac events, were recorded at the time of onset. When a patient was transferred to another department or hospital, the investigator recorded adverse event data from the department or hospital as much as possible. When a patient did not visit the investigator’s institute, the investigator asked him/her the reason for not visiting and whether adverse events had occurred.
Outcome measures
The primary endpoint of this survey was defined as a cerebrovascular or cardiac event. Cerebrovascular events included the following: the onset or recurrence of cerebral hemorrhage, subarachnoid hemorrhage or cerebral infarction, which were diagnosed on the basis of unequivocal signs or symptoms of the neurological deficit that had a sudden onset and a duration of more than 24 h, or on the basis of computed tomography or magnetic resonance imaging findings; or transient ischemic attack, which was defined as a focal neurological deficit lasting for <24 h. Cardiac events included the following: the onset or recurrence of myocardial infarction, which was diagnosed on the basis of typical clinical symptoms (ischemic chest pain, pulmonary edema or carcinogenic shock), electrocardiogram changes (development of pathological Q wave, ST-T segment elevation or depression, or new left bundle branch block) and cardiac enzyme elevation;10, 11 angina pectoris, which was diagnosed on the basis of chest pain or discomfort, and electrocardiograph changes; asymptomatic myocardial ischemia, which was diagnosed by exercise testing or nuclear imaging studies; or heart failure, including an acute onset and worsening chronic status, which was diagnosed on the basis of clinical symptoms (shortness of breath, leg fatigue, edema or orthopnea), echocardiography findings (left ventricular systolic dysfunction defined as an ejection fraction of <40%) or elevated levels of biomarkers such as brain natriuretic peptide.12, 13, 14 The first of these events to arise in a patient was considered the primary endpoint. The primary endpoint also included death caused by the above events. Diagnosis of the conditions listed above was performed by the investigators who participated in this survey according to the criteria mentioned above.
Data analysis
The following risk factors for cardiovascular diseases were collected as background information on the patients: history or complications of dyslipidemia, diabetes, left ventricular hypertrophy, angina pectoris, myocardial infarction, heart failure, cerebral hemorrhage, cerebral infarction, transient ischemic attack, proteinuria, renal impairment, renal failure, arteriosclerotic plaque, aortic dissection, occlusive arterial disease or hypertensive retinopathy. For data analysis, cerebral hemorrhage, cerebral infarction and transient ischemic attack were classified as cerebrovascular disease; left ventricular hypertrophy, angina pectoris, myocardial infarction and heart failure were classified as cardiovascular disease; proteinuria, renal impairment and renal failure were classified as renal disease; and arteriosclerotic plaque, aortic dissection and occlusive arterial disease were classified as vascular disease. We analyzed the relationship between cerebrovascular and cardiac events and the following factors as a pre-specified objective: sex, age (<65 years or >65 years), risk factors mentioned above, cigarette smoking and additional antihypertensive agents. Additionally, the relationship between cerebrovascular and cardiac events and BP at the endpoint as measured at the last visit or before the occurrence of an event was analyzed as a post hoc objective. For safety evaluation, adverse drug reactions were defined as adverse events that were not denied causality for valsartan by the investigators.
Statistical analysis
The number of subjects in the analysis set was determined such that cerebrovascular and cardiac events would be detected in each of the following three groups with risk factors for cardiovascular disease in hypertensive patients (JSH 2000):15 (1) patients without risk factors; (2) patients with risk factors other than diabetes; and (3) patients with diabetes, organ damage or cardiovascular disease. Thus, these risk factor groups were estimated to account for 15, 20 and 65% of hypertensive patients, respectively, as shown in the Study Group on Long-Term Antihypertensive Therapy (GLANT).16 To detect at least one cerebrovascular or cardiac event that occurs at a rate of 0.1 with a 95% confidence interval, the number of subjects would be 3000. To collect one event among patients with no risk factors of which the prevalence was 15%, at least 3000 patients without risk factors should be enrolled. Thus, 20 000 subjects would be necessary to assess the above-mentioned hypothesis.
The analysis set consisted of patients who were enrolled in the survey and given valsartan. The incidences of cerebrovascular events, cardiac events and cerebrovascular/cardiac events (combination of cerebrovascular and cardiac events) were calculated by the Kaplan–Meier method. A Cox proportional hazards model was used to search for factors that might affect the onset of cerebrovascular and cardiac events, and one-way analysis of variance was used to assess changes in BP and pulse rate. For the calculation of the adjusted hazard ratio, the following factors were used as covariates: sex, age and the existence risk factors. The data are expressed as the mean value±s.d., and the level of significance was set at P<0.05.
Results
Patient characteristics
Of the 30 366 patients who received valsartan-based therapy that were enrolled in the survey from 2940 institutions, the data from 29 059 patients were collected by December 2007. Of the 29 059 patients whose data were collected, 565 did not revisit after receiving the first dose of valsartan, and 46 of them were excluded from the analysis because of violation of the enrollment requirements and 28 because of unidentified adverse events. As a result, 28 420 patients were eligible for inclusion in the safety analysis, and 64 of these were excluded from the event analysis because they failed to be reported an observation end date. Thus, 28 356 were evaluable for the event analysis. The median duration of the observation period was 2.93 years, and data for 59 208 patient-years were collected.
Table 1 shows the characteristics of the 28 356 patients who were included in the event analysis. The percentages of men and women were 50.8 and 49.2%, respectively, and the mean age was 64.6±12.0 years. Patients aged 65 years or older accounted for 53.1%. The following risk factors and past histories were observed: dyslipidemia (32.6%), diabetes (20.2%), cerebrovascular disease (9.7%), cardiovascular disease (18.7%), renal disease (8.3%), vascular disease (2.9%) and hypertensive retinopathy (0.7%). The percentage of patients with a history of smoking was 27.6%.
The dose of valsartan was significantly increased from 71.8±21.7 mg at the start to 77.5±27.3 mg at endpoint (P<0.001, Table 2). The percentage of patients not receiving concomitant antihypertensive drugs at the start of the survey was 50.3%, which decreased to 43.2% at the endpoint. Antihypertensive drugs other than valsartan were added for 2015 patients (7.1%), and of the drugs added, Ca-blockers and diuretics were the most frequently used, followed by α-blockers (Table 2). Eventually, 43.2% of patients were treated with valsartan alone.
BP and pulse rate
Figure 1 shows the changes in BP and pulse rate. Both systolic and diastolic BP significantly decreased after the administration of valsartan from 161.1±19.1/90.4±13.1 to 139.9±18.1/79.6±11.9 mm Hg. In patients treated with valsartan alone (mono treatment group), the BP decreased from 160.5±17.9/91.2±12.2 to 139.3±17.6/80.3±11.5 mm Hg (P<0.001). In patients treated with valsartan in addition to other drugs (add-on treatment group), the BP decreased from 161.6±19.9/89.7±13.7 to 139.5±18.0/78.6±11.8 mm Hg (P<0.001). Although there was no significant difference in the systolic BP at the endpoint between the two groups, there was a slight, but significant, difference in the diastolic BP at the endpoint between the groups (P<0.001). The distribution of diastolic BP at the endpoint was 80 (72, 78) mm Hg (described as median (25 and 75% tiles)) in the mono treatment group and 80 (70, 86) mm Hg in the add-on treatment group, respectively. This means that both distributions were similar. The pulse pressure significantly decreased from 69.3±0.1 to 59.0±0.1 mm Hg in the mono treatment group and from 71.9±0.1 to 60.9±0.1 mm Hg in the add-on treatment group, respectively, and there was a significant difference in the pulse pressure at the endpoint between both groups (P<0.001). The percentage of patients attaining an initial target BP of <140/90 mm Hg at the endpoint was 50.5%. The pulse rate was slightly, but significantly, decreased from 74.7±11.6 to 73.3±10.8 beats per min at the endpoint (P<0.001).

Changes in BP and pulse rate. Administration of valsartan significantly decreased both systolic and diastolic BP (P<0.001, analysis of variance), as shown in the upper panel. The pulse rate was slightly but significantly decreased (P<0.001, analysis of variance), as shown in the lower panel. Data are expressed as the mean value±s.d.
Cerebrovascular and cardiac events
Cerebrovascular events were observed in 550 patients (1.94%, 9.29/1000 patient-years), and cardiac events were observed in 576 patients (2.03%, 9.73/1000 patient-years). Two patients had both cerebrovascular and cardiac events concurrently, and 1124 patients had either one or the other (3.96%, 18.98/1000 patient-years). The cerebrovascular events observed were cerebral infarction (n=360), cerebral hemorrhage (n=80), transient ischemic attack (n=95), and subarachnoid hemorrhage (n=22). The cardiac events observed were angina pectoris (n=246), heart failure (n=212), myocardial infarction (n=119) and asymptomatic myocardial ischemia (n=23). Cerebrovascular and cardiac death was observed in 135 patients (0.48%, 2.28/1000 patient-years). Figure 2 shows the Kaplan–Meier curves of the cerebrovascular and cardiac events.

Kaplan–Meier curves of cerebrovascular/cardiac events (a), cerebrovascular events (b) and cardiac events (c).
Table 3 shows the incidences and hazard ratios for cerebrovascular and cardiac events according to the demographic characteristics of patients. Men were at a greater risk than women. All of the factors other than dyslipidemia and hypertensive retinopathy were significant risk factors for cerebrovascular/cardiac events. A comparison of cerebrovascular and cardiac events revealed that dyslipidemia was more likely to be a risk factor for cardiac events than for cerebrovascular events. Other common risk factors presented a similar risk in both events.
The adjusted hazard ratios for cerebrovascular and cardiac events were compared among the patients with four BP levels at baseline (normal BP and stage I–III hypertension). The BP at baseline was not a significant related factor for cerebrovascular events (P=0.285) or cardiac events (P=0.332).
Because the BP at the endpoint was not determined in 87 patients, the relationship between cerebrovascular/cardiac events and final BP was investigated in 28 269 patients. Table 4 shows the adjusted hazard ratios for cerebrovascular and cardiac events by BP level at the endpoint. Both ⩾140 mm Hg in systolic BP and ⩾90 mm Hg in diastolic BP were stronger risk factors for both cerebrovascular and cardiac events. As shown in Figure 3, the risk of developing cerebrovascular and cardiac events (adjusted hazard ratio) increased linearly in an age-dependent manner.

The 95% confidence interval (CI) and adjusted hazard ratios for cerebrovascular events (○) and cardiac events (•) by age (a), systolic BP (b) and diastolic BP (c).
Regarding cerebrovascular events, a risk reduction depending on the systolic and diastolic BPs was observed, and the risk was significantly high with a systolic BP of ⩾140 mm Hg or a diastolic BP of ⩾80 mm Hg (Figure 3). Regarding cardiac events, a clear risk reduction related to BP was not found; however, the risk was significantly higher in patients with a systolic BP of ⩾150 mm Hg or a diastolic BP of⩾90 mm Hg (Figure 3).
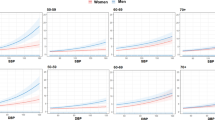
Table 5 shows the adjusted hazard ratios for cerebrovascular and cardiac events by both age and BPs at the endpoint. The risk of developing cerebrovascular events was significantly increased with a systolic BP of ⩾150 mm Hg or a diastolic BP of ⩾90 mm Hg in patients aged <65 years and with a systolic BP of ⩾140 mm Hg or a diastolic BP of ⩾85 mm Hg in patients aged ⩽65 to <75 and in patients aged ⩾75 years. Regarding cardiac events, a weak J-curve phenomenon was observed for the systolic BP only in patients aged ⩾75 years (Figure 4).

The 95% confidence interval (CI) and adjusted hazard ratios for cerebrovascular events (a, b) and cardiac events (c, d) by <65 (○), ⩾65 to <75 (◊) and ⩾75 (▴) patients.
Safety
Adverse drug reactions were observed in 1925 of 28 420 patients (6.77%), and the number of cases of adverse drug reactions was 2497 (8.79%). The major adverse drug reactions were excess decrease in BP (268 cases), dizziness (203 cases), headache (78 cases) and hyperkalemia (71 cases). Adverse drug reactions according to the System Organ Class are listed in Table 6.
Discussion
We analyzed data from 28 356 patients (mean age: 64.6 years) obtained from the designated drug use investigation of valsartan that was conducted as post-marketing surveillance in accordance with Japanese government regulations. Administration of valsartan significantly reduced systolic and diastolic BP, and slightly, but significantly, decreased pulse rate. For both cerebrovascular and cardiac events, advanced age (⩾65 years), past history of cardiovascular diseases and cigarette smoking were significant risk factors. A higher BP achieved after treatment was a strong risk factor for the incidence of cerebrovascular events, which were significantly high in patients with a systolic BP of ⩾140 mm Hg or a diastolic BP of ⩾80 mm Hg. Regarding cardiac events, the risk was significantly high with a systolic BP of ⩾150 mm Hg or a diastolic BP of ⩾90 mm Hg, and a weak J-curve phenomenon was observed for the systolic BP in elderly patients (⩾75 years).
Persistently high BP is a cause of vascular disorders and a risk factor for the development or progression of major organ damage. Additional layering of risk factors such as dyslipidemia and diabetes increases the incidence of cerebrovascular and cardiovascular events exponentially.17, 18 In the present survey, advanced age (⩾65 years), cigarette smoking and diabetes were significant risk factors, as stated in JSH 2009.5 The hazard ratios for cerebrovascular and cardiac events in the elderly versus the nonelderly patients were 2.62 and 2.71, respectively. The hazard ratios for the events in smokers versus non-smokers were 1.38. Thus, there was no difference between the hazard ratios for both events. The hazard ratios for the cerebrovascular and cardiac events in patients with diabetes versus those without, however, were 1.50 and 1.79, respectively, indicating that diabetes was a stronger risk factor for cardiac events than for cerebrovascular events. Furthermore, comparison of patients with and without organ damage showed that cerebrovascular disease was a stronger risk factor for cerebrovascular events, and renal disease and cardiovascular disease were stronger risk factors for cardiac events. Similar findings were also reported in national observational studies,19, 20 and the results of the present survey coincided well with those that have been previously reported.
Analysis of the demographic characteristics of the patients revealed that complications were more likely to be risk factors than the baseline BP. In clinical trials comparing antihypertensive drugs, it was reported that differences in the achieved BP affected the therapeutic outcomes.21, 22 Therefore, evaluating the relationship between BP levels at the endpoint and the incidence of cerebrovascular and cardiac events was considered reasonable. Observational studies of the relationship between BP and cerebrovascular and cardiovascular events showed that there was a linear relationship between cerebrovascular events and BP, and cerebral hemorrhage was more strongly related to BP than cerebral infarction.23 It was also reported that there was a weaker relationship between cardiac events and BP,24 and the relationship between BP and each type of events was weakened with age.25 With regard to interventional studies, a meta-analysis suggests that the greater the degree of BP reduction, the greater the benefit for lowering the risk of composite cardiovascular endpoints.26 However, the meta-analysis does not take into account the achieved BP in those studies, and another meta-analysis performed by the same group suggests that while treating hypertension reduces the risk of both stroke and myocardial infarction in hypertensive diabetes mellitus patients overall, when a lesser degree of BP control is compared with a higher degree of control (an achieved systolic BP of 139 mm Hg versus 129 mm Hg), the reduction in the risk of myocardial infarction was not significantly decreased, but a significant reduction in stroke was observed.27 Similarly, in the present survey, there was a linear relationship between the incidence of cerebrovascular events and BP, suggesting that the hypothesis of ‘the lower, the better’ was correct. The increasing risk associated with both systolic and diastolic BP for cardiac events was weaker than that for cerebrovascular events, and the J-curve phenomenon in elderly patients (⩾75 years) was observed for cardiac events only for systolic BP. However, a systolic BP of ⩾150 mm Hg and a diastolic BP of ⩾90 mm Hg were stronger risk factors than a systolic BP <120 mm Hg and a diastolic BP <70 mm Hg. Sub-analysis of several clinical trials has revealed the J-curve phenomenon.28, 29
The underlying cause of the J-curve phenomenon and the relationship between BP and cardiac events in elderly patients remains controversial. Because coronary perfusion pressure is maintained by diastolic BP, coronary blood flow cannot be maintained if the diastolic and systolic BP decrease in patients with coronary artery stenosis, left ventricular hypertrophy and other conditions.30 This may be the reason for the significantly high incidence of cardiac events in patients with a history of cardiovascular disease. In the elderly, the physiological response to maintain coronary blood flow, as well as other organ blood flow, against BP deteriorate due to reduction of vascular compliance.31 This may be also associated with the J-curve phenomenon observed in elderly patients in this survey.
A decrease in BP was epidemiologically reported to be a marker for underlying poor health and subsequent mortality in older adults.32 In addition, meta-analysis of individual patient’s data from seven randomized clinical trials demonstrated that the J-curve phenomenon between BP and cardiovascular events was observed in patients treated with antihypertensive drugs and in non-treated patients.33 These results suggest that the J-curve phenomenon is not caused by treatment with antihypertensive drugs, but rather caused by poor health conditions. From this survey, the interpretation of the J-curve phenomenon is difficult because a target BP to be achieved was not set in this survey, and there are many modulating factors besides BP that may affect cerebrovascular and cardiac events.34 Considering complications as risk factors, the prevalence of high-risk patients with a history of cardiovascular diseases was higher in the lowest BP category, systolic BP <120 mm Hg or diastolic BP <70 mm Hg at the endpoint compared with the other categories. However, a similar result was not found in patients with cerebrovascular diseases (Supplementary Table). Thus, the J-curve phenomenon may result from the high prevalence of high-risk patients with systolic BP <120 mm Hg. This finding also suggests that the BP in high-risk patients with cardiovascular disease may be decreased more easily. Further study is needed to clarify the mechanism of the J-curve phenomenon observed in the present study.
The question of the optimal BP target in antihypertensive treatment is related to the J-curve phenomenon. Few studies have actually shown that ‘lower is better’ for reducing cardiovascular events with antihypertensive treatment, especially for patients with a systolic BP of <130 mm Hg. The Studio Italiano Sugli Effetti Cardiovascolari del Controllo della Pressione Arteriosa Sistolica (Cardio-Sis) trial compared a target systolic BP of <140 mm Hg with a target systolic BP of <130 mm Hg in hypertensive patients without diabetes mellitus and revealed that targeting a systolic BP of <130 mm Hg significantly reduced the rate of left ventricular hypertrophy compared with targeting a systolic BP of <140 mm Hg.35 It also showed, as its main secondary outcome, that the composite cardiovascular endpoints were significantly reduced in the systolic BP <130 mm Hg targeted group. However, left ventricular hypertrophy diagnosed by electrocardiogram is a surrogate endpoint for cardiovascular endpoint, and most of the cardiovascular events that contributed to the difference between the two target groups were coronary revascularization and new-onset atrial fibrillation, which are ‘softer’ endpoints compared with endpoints such as stroke, myocardial infarction or death. Thus, taken together with the results of our survey, further investigation would be needed to clarify the optimal BP level for reducing cardiovascular events.
Regarding the incidences of cerebrovascular and cardiac events, which was 9.29/1000 patient-years for cerebrovascular events and 2.01/1000 patient-years for myocardial infarction in this survey, it was reported that the incidence of cerebrovascular events and myocardial infarction were 3.90/1000 and 1.02/1000 patient-years in the Japan Hypertension Evaluation with Angiotensin II Antagonist Losartan Therapy study (J-HEALTH),36 and 7.4/1000 and 2.7/1000 patient-years in Practitioner’s Trial on the Efficacy of Antihypertensive Treatment in Elderly Patients with Hypertension II study (PATE-Hypertension).37 Both surveys were single-arm anti hypertensive studies conducted in Japan similar to this survey. Although the incidence rates were different among the surveys, which may be explained by differences in the patients’ background, cerebrovascular events tended to occur much more frequently than myocardial infarction in all of the studies. On the other hand, the incidences of stroke and myocardial infarction in Valsartan Antihypertensive Long-term Use Evaluation (VALUE)38 were 10.0/1000 patient-years for stroke and 11.4/1000 patient-years for myocardial infarction, showing a relatively higher ratio of cardiac to cerebrovascular incidence rates compared with the surveys mentioned above. This result may reflect the lower incidence rate of coronary heart disease in the general Japanese population than the Western population.39, 40 However, VALUE was a randomized control study performed on patients with high cardiovascular risk, and the comparison of incidence rates warrants careful interpretation.
Regarding adverse drug reactions, most of them were tolerable and described in the package insert of valsartan. Additionally, the incidence ratio and types of adverse drug reactions reported in this survey were similar to those of another post marketing surveillance of valsartan with 7258 patients (data not shown). These findings indicated that valsartan is a well-tolerated antihypertensive agent.
There were several limitations of this survey. In particular, 2010 of 30 366 patients (6.6%) were excluded for the reasons mentioned above; the main reason was that data collection were not completed by the deadline of December 2007. Secondarily, the data were collected from a non-randomized observational survey without any interventional limits and with no control group. Additionally, the reported endpoints, cerebrovascular and cardiac events, were not evaluated by other independent investigators. The findings from the analysis of the subgroups and BP classifications have limitations, although the data were adjusted for patient demographic factors; sex, age and the existence risk factors. However, this survey provides a valuable database due to the relatively large sample size, which contains clinical information. Because the target BP required to reduce the incidence of cardiovascular events remains controversial,41, 42 further investigations are required.
The results of the investigation of valsartan use with a sample size of about 28 000 revealed the following: (1) Valsartan, alone or in combination with other antihypertensive drugs, was effective at controlling BP. (2) In patients receiving antihypertensive treatment with valsartan, the incidence of cerebrovascular/cardiovascular events, cerebrovascular events and cardiac events was 18.98/1000, 9.29/1000 and 9.73/1000 patient-years, respectively. (3) There was a linear relationship between cerebrovascular events, and the systolic and diastolic BP levels at any age and less of a relationship between cardiac events and systolic and diastolic BP. However, a weak J-curve phenomenon was observed in the relationship between cardiac events and systolic BP only in elderly hypertensive patients (⩾75 years). Further study is needed to clarify the mechanism of the J-curve phenomenon. (4) Valsartan is a well-tolerated antihypertensive agent, similar to other ARBs.
References
Chobanian AV, Bakris GL, Black HR, Cushman WC, Green LA, Izzo JL, Jones DW, Materson BJ, Oparil S, Wright JT, Roccella EJ ; National Heart, Lung, and Blood Institute Joint National Committee on Prevention, Detection, Evaluation, and Treatment of High Blood Pressure; National High Blood Pressure Education Program Coordinating Committee. The seventh report of the Joint National Committee on prevention, detection, evaluation, and treatment of high blood pressure: the JNC-7 Report. JAMA 2003; 289: 2560–2572.
Veterans Administration cooperative study group on antihypertensive agents. Effects of treatment on morbidity in hypertension; results in patients with diastolic blood pressures averaging 115 through 129mm Hg. JAMA 1967; 202: 1028–1034.
Staessen JA, Fagard R, Thijs L, Celis H, Arabidze GG, Birkenhäger WH, Bulpitt CJ, de Leeuw PW, Dollery CT, Fletcher AE, Forette F, Leonetti G, Nachev C, O'Brien ET, Rosenfeld J, Rodicio JL, Tuomilehto J, Zanchetti A . Randomised double-blind comparison of placebo and active treatment for older patients with isolated systolic hypertension. The systolic hypertension in Europe (Syst-Eur) trial investigators. Lancet 1997; 350: 757–764.
Dahlöf B, Devereux RB, Kjeldsen SE, Julius S, Beevers G, de Faire U, Fyhrquist F, Ibsen H, Kristiansson K, Lederballe-Pedersen O, Lindholm LH, Nieminen MS, Omvik P, Oparil S, Wedel H ; LIFE Study Group. Cardiovascular morbidity and mortality in the Losartan Intervention For Endpoint reduction in hypertension study (LIFE): a randomised trial against atenolol. Lancet 2002; 359: 995–1003.
The Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension. Guidelines for the Management of Hypertension 2009. Life Science Publishing: Tokyo. 2009.
Summary of Vital Statistics: trends in leading causes of death, Vital Statistics, Ministry of Health, Labour and Welfare, Japan, 2010. http://www.mhlw.go.jp/toukei/saikin/hw/jinkou/suii02/deth7.html . Accessed on April 27 2012.
Mori H, Ukai H, Yamamoto H, Saitou S, Hirao K, Yamauchi M, Umemura S . Current status of antihypertensive prescription and associated blood pressure control in Japan. Hypertens Res 2006; 29: 143–151.
Kannel WB . Histolic perspectives on the relative contributions of diastolic and systolic blood pressure elevation to cardiovascular risk profile. Am Heart J 1999; 138 (3 part 2): 205–210.
Cristione L, Gasparo M, Buhlmayer P, Whitebread S, Ramojoune H, Wood J . Pharmacological profile of valsartan: a potent, orally active, nonpeptide antagonist of the angiotensin II AT1-receptor subtype. Br J Pharmacol 1993; 110: 761–771.
The Japanese Circulation Society.. Guidelines for the management of patients with ST-elevation myocardial infarction (JCS 2008). http://www.j-circ.or.jp/guideline/pdf/JCS2008_takano_h.pdf . Accessed on April 27 2012.
Thygesen K, Alpert JS, White HD . Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction, Universal definition of myocardial infarction. Circulation 2007; 116: 2634–2653.
The Japanese Circulation Society.. Guidelines for Treatment of Acute Heart Failure (JCS 2011). http://www.j-circ.or.jp/guideline/pdf/JCS2011_izumi_h.pdf . Accessed on April 27 2012.
McKee PA, Castelli WP, McNamara PM, Kannel WB . The natural history of congestive heart failure: the Framingham study. N Engl J Med 1971; 285: 1441–1446.
Kim J, Jacobs DR, Luepker RV, Shahar E, Margolis KL, Becker MP . Prognostic value of a novel classification scheme for heart failure: the Minnesota Heart Failure Criteria. Am J Epidemiol 2006; 164: 184–193.
The Japanese Society of Hypertension Committee for Guidelines for the Management of Hypertension.. Guidelines for the Management of Hypertension 2000 (JSH 2000). Japanese Society of Hypertension: Tokyo,. 2000.
The GLANT study group. A 12-month comparison of ACE inhibitor and Ca antagonist therapy in mild to moderate essential hypertension; the GLANT study. Hypertens Res 1995; 18: 235–244.
Prospective Studies Collaboration; Lewington S, Whitlock G, Clarke R, Sherliker P, Emberson J, Halsey J, Qizilbash N, Peto R, Collins R . Blood cholesterol and vascular mortality by age, sex, and blood pressure: a meta-analysis of individual data from 61 prospective studies with 55,000 vascular deaths. Lancet 2007; 370: 1829–1839.
Kadota A, Hozawa A, Okamura T, Kadowak T, Nakmaura K, Murakami Y, Hayakawa T, Kita Y, Okayama A, Nakamura Y, Kashiwagi A, Ueshima H ; NIPPON DATA Research Group. Relationship between metabolic risk factor clustering and cardiovascular mortality stratified by high blood glucose and obesity: NIPPON DATA90, 1990-2000. Diabetes Care 2007; 30: 1533–1538.
Fujishima M, Kiyohara Y, Kato I, Ohmura T, Iwamoto H, Nakayama K, Ohmori S, Yoshitake T . Diabetes and cardiovascular disease in a prospective population survey in Japan: the Hisayama study. Diabetes 1996; 45 (Suppl 3): S14–S16.
Ninomiya T, Kiyohara Y, Kubo M, Tanizaki Y, Doi Y, Okubo K, Wakugawa Y, Hata J, Oishi Y, Shikata K, Yonemoto K, Hirakata H, Iida M . Chronic kidney disease and cardiovascular disease in a general Japanese population: the Hisayama Study. Kidney Int 2005; 68: 228–236.
Staessen JA, Wang JG, Thijs L . Cardiovascular prevention and blood pressure reduction: a quantitative overview updated until 1 March 2003. J Hypertens 2003; 21: 1055–1076.
Blood Pressure Lowering Treatment Trialists' Collaboration; Turnbull F, Neal B, Pfeffer M, Kostis J, Algert C, Woodward M, Chalmers J, Zanchetti A, MacMahon S . Blood pressure-dependent and independent effects of agents that inhibit the renin-angiotensin system. J Hypertens 2007; 25: 951–958.
Rashid P, Leonardi-Bee J, Bath P . Blood pressure reduction and secondary prevention of stroke and other vascular events: a systematic review. Stroke 2003; 34: 2741–2748.
Lawes CM, Rodgers A, Bennett DA, Parag V, Suh I, Ueshima H, MacMahon S ; Asia Pacific Cohort Studies Collaboration. Blood pressure and cardiovascular disease in the Asia Pacific region. J Hypertens 2003; 21: 707–716.
Okayama A, Kadowaki T, Okamura T, Hayakawa T, Ueshima H ; The NIPPON DATA80 Research Group. Age-specific effects of systolic and diastolic blood pressures on mortality due to cardiovascular diseases among Japanese men (NIPPON DATA80). J Hypertens 2006; 24: 459–462.
Verdecchia P, Gentile G, Angeli F, Mazzotta G, Mancia G, Reboldi G . Influence of blood pressure reduction on composite cardiovascular endpoints in clinical trials. J Hypertens 2010l; 28: 1356–1365.
Reboldi G, Gentile G, Angeli F, Ambrosio G, Mancia G, Verdecchia P . Effects of intensive blood pressure reduction on myocardial infarction and stroke in diabetes: a meta-analysis in 73 913 patients. J Hypertens 2011; 29: 1253–1269.
Sleight P, Redon J, Verdecchia P, Mancia G, Gao P, Fagard R, Schumacher H, Weber M, Böhm M, Williams B, Pogue J, Koon T, Yusuf S ; ONTARGET investigators. Prognostic value of blood pressure in patients with high vascular risk in the ongoing telmisartan alone and in combination with ramipril global endpoint trial study. J Hypertens 2009; 27: 1360–1369.
Hansson L, Zanchetti A, Carruthers SG, Dahlöf B, Elmfeldt D, Julius S, Ménard J, Rahn KH, Wedel H, Westerling S . Effects of intensive blood-pressure lowering and low-dose aspirin in patients with hypertension: principal results of the hypertension optimal treatment (HOT) randomised trial. HOT study group. Lancet 1998; 351: 1755–1762.
Rosendorff C, Black HR . Evidence for a lower target blood pressure for people with heart disease. Curr Opin Cardiol 2009; 24: 318–324.
Lim MA, Townsend RR . Arterial compliance in the elderly: its effect on blood pressure measurement and cardiovascular outcomes. Clin Geriatr Med 2009; 25: 191–205.
Satish S, Zhang DD, Goodwin JS . Clinical significance of falling blood pressure among older adults. J Clin Epidemiol 2001; 54: 961–967.
Boutitie F, Gueyffier F, Pocock S, Fagard R, Boissel JP . J-shaped relationship between blood pressure and mortality in hypertensive patients: new insights from a meta-analysis of individual-patient data. Ann Intern Med 2002; 136: 438–448.
Hedner T, Oparil S, Narkiewicz K, Kjeldsen SE . The J-curve phenomenon revisited. Blood Press 2009; 18: 168–170.
Verdecchia P, Staessen JA, Angeli F, de Simone G, Achilli A, Ganau A, Mureddu G, Pede S, Maggioni AP, Lucci D, Reboldi G ; Cardio-Sis investigators. Usual versus tight control of systolic blood pressure in non-diabetic patients with hypertension (Cardio-Sis): an open-label randomised trial. Lancet 2009; 374: 525–533.
Shimamoto K, Fujita T, Ito S, Naritomi H, Ogihara T, Shimada K, Tanaka H, Yoshiike N ; J-HEALTH Study Committees.. Impact of blood pressure control on cardiovascular events in 26 512 Japanese hypertensive patients: the Japan Hypertension Evaluation with Angiotensin II Antagonist Losartan Therapy (J-HEALTH) study, a prospective nationwide observational study. Hypertens Res 2008; 31: 469–478.
Ogihara T, Matsuoka H, Rakugi H . Practitioner’s trial on the efficacy of antihypertensive treatment in elderly patients with hypertension II (PATE-hypertension II study) in Japan. Geriatr Gerontol Int 2011; 11: 414–421.
Julius S, Kjeldsen SE, Weber M, Brunner HR, Ekman S, Hansson L, Hua T, Laragh J, McInnes GT, Mitchell L, Plat F, Schork A, Smith B, Zanchetti A ; VALUE trial group. Outcomes in hypertensive patients at high cardiovascular risk treated with regimens based on valsartan or amlodipine: the VALUE randomised trial. Lancet 2004; 363: 2022–2031.
Verschuren WM, Jacobs DR, Bloemberg BP, Kromhout D, Menotti A, Aravanis C, Blackburn H, Buzina R, Dontas AS, Fidanza F, Karvonen MJ, Nedelijković S, Nissinen A, Toshima H . Serum total cholesterol and long-term coronary heart disease mortality in different cultures: twenty-five—year follow-up of the seven countries study. JAMA 1995; 274: 131–136.
Saito I, Folsom AR, Aono H, Ozawa H, Ikebe T, Yamashita T . Comparison of fatal coronary heart disease occurrence based on population surveys in Japan and the USA. Int J Epidemiol 2000; 29: 837–844.
Messerli FH, Panjrath GS . The J-curve between blood pressure and coronary artery disease or essential hypertension: exactly how essential? J Am Coll Cardiol 2009; 54: 1827–1834.
Grossman E . Blood pressure: the lower, the better: the con side. Diabetes Care 2011; 34 (Suppl 2): S308–S312.
Acknowledgements
We gratefully thank the physicians and staff at the 2940 participating institutions for their contributions to this survey. The authors also thank Drs Kazuaki Shimamoto, Kazuyuki Shimada and Toshio Ogihara for their critical comments. This survey was funded and conducted by Novartis Pharma KK for post-marketing surveillance.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies the paper on Hypertension Research website
Supplementary information
Rights and permissions
About this article
Cite this article
Yamazaki, T., Kohro, T., Chujo, M. et al. The occurrence rate of cerebrovascular and cardiac events in patients receiving antihypertensive therapy from the post-marketing surveillance data for valsartan in Japan (J-VALID). Hypertens Res 36, 140–150 (2013). https://doi.org/10.1038/hr.2012.154
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/hr.2012.154
Keywords
This article is cited by
-
Association between blood pressure and disability-free survival among community-dwelling elderly patients receiving antihypertensive treatment
Hypertension Research (2014)
-
Pharmacotherapy for Hypertension in Older Adults: A Systematic Review
Drugs & Aging (2014)
-
Hypertension and the J-curve phenomenon: implications for tight blood pressure control
Hypertension Research (2013)
