
Abstract
Purpose:
There is debate within the genetics community about the optimal term to describe genetic variants unrelated to the test indication but potentially important for health. Given the lack of consensus and the importance of adopting terminology that promotes effective clinical communication, we sought the opinion of clinical genetics patients.
Methods:
Surveys and focus groups with two patient populations were conducted. Eighty-eight survey participants were asked to rank four terms according to how well each describes results unrelated to the test indication: incidental findings, secondary findings, additional findings, and ancillary findings. Participants in six focus groups were guided through a free-thought exercise to describe the desired attributes of such a term and then asked to formulate the best term to represent this concept.
Results:
The term additional findings had the most first-choice rankings by survey participants, followed by secondary findings, incidental findings, and ancillary findings. Most focus group participants preferred the term additional findings; they also gave reasons why other terms were not optimal.
Conclusion:
Additional findings was preferred because it was more neutral and accessible than other terms currently in use. Patient perceptions and comprehension will be framed by the terminology used by healthcare providers. Thus, patient opinions should be considered by medical genetics professionals.
Genet Med 19 2, 176–181.
Similar content being viewed by others

Introduction
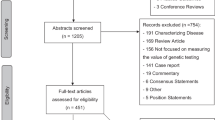
As technology advances, genomic sequencing is becoming a more accessible and reliable tool for characterizing the molecular nature of disease, leading to the increasing use of large-scale sequencing tests such as multigene panels, exome sequencing, and genome sequencing. Large-scale sequencing may uncover variants of potential clinical significance unrelated to the disease that prompted the evaluation. In other words, these variants may be related to risks of developing a different disease(s) or they may identify carrier status for recessive diseases. For example, an exome sequencing test performed for a neurological disorder with unknown etiology may identify a pathogenic variant in MYBPC3 associated with increased risk of hypertrophic cardiomyopathy. Individuals in the clinical genetics community commonly refer to these types of results as incidental findings. This terminology arose because of similarities to other medical contexts, such as radiologists identifying atypical or abnormal imaging findings unrelated to a presenting condition (e.g., a thyroid mass on a chest radiograph performed for shortness of breath1). However, the American College of Medical Genetics and Genomics (ACMG) recommendations for reporting incidental findings in clinical exome and genome sequencing define incidental findings as “the results of a deliberate search for pathogenic or likely pathogenic alterations in genes that are not apparently relevant to a diagnostic indication for which the sequencing test was ordered.”2 Thus, in the context of genomics, informatics may be used to include (or exclude) specific variants unrelated to the indication for testing and the identification of these findings is quite different from the incidental findings of other medical specialties.
For this and other reasons, terms other than incidental findings have made their way into the lexicon; the terms secondary variants unexpected results unsolicited findings unrelated findings and nonpertinent findings have all been proposed.3,4,5,6,7,8,9 Although the relative merits and potential controversy regarding some of these terms have been reviewed,10,11 we are not aware of a study that has sought data on patient preferences in this regard. It is essential to identify patient preferences because the language that clinicians use to explain these types of results has the potential to promote effective patient decision making or cause confusion or misperceptions about the nature of the findings, thus undermining effective patient decision making. Here, we present the results of the following two studies of two patient populations as part of the Clinical Sequencing Exploratory Research (CSER) consortium: (i) a survey of University of Washington (UW) Division of Medical Genetics patients’ perspectives and preferences regarding terminology used to describe genetic findings unrelated to the test indication and (ii) data from focus groups conducted by investigators at the University of North Carolina (UNC) at Chapel Hill regarding patient reactions to the term incidental findings.
Materials and Methods
The terminology question was raised in the context of the National Human Genome Research Institute/National Cancer Institute–funded CSER consortium, which is exploring the integration of genomic sequencing technology into clinical care.12 Two CSER consortium projects independently explored this issue in the context of their studies.
The CSER UW New Exome Technology (NEXT) in Medicine study is a randomized controlled trial targeting individuals who presented to medical genetics for testing related to colorectal cancer. The study compares two arms: (i) usual clinical care genetic testing for hereditary colorectal cancer/polyps (CRCP) (usual care group) and (ii) usual clinical care genetic testing for CRCP plus exome sequencing (exome sequencing group).13 Participants receive diagnostic as well as other types of genomic findings. The CSER UNC North Carolina Clinical Genomic Evaluation by NextGen Exome Sequencing (NCGENES) study is investigating best practices for using exome sequencing for clinical diagnoses in adult and pediatric patients who have symptoms or a condition with a suspected genetic etiology that has not yet been identified. NCGENES participants also receive additional genomic findings.
Development of survey and focus group materials
A survey to explore terminology preferences in the UW adult genetics population was developed by UW medical genetics faculty, a genetic counselor, a medical student, and a research coordinator. The concept of incidental findings was defined in the survey as “gene changes that are not related to the initial reason the clinic ordered the genetic test, but may be important for the patient’s health care.” Four terms were selected from the literature by the interdisciplinary UW team and participants were asked to rank them: incidental findings, secondary findings, additional findings, and ancillary findings. Participants were also asked, “How strongly do you feel there are better and worse choices?” on a scale of 1 (it does not matter) to 5 (some are better). They also had the option to suggest a different term. Basic demographic information was also collected, including sex, age group, race, and ethnicity. A paper survey and an electronic survey were developed. Terms were presented in a randomized order in the electronic survey to evaluate if the order in which the terms were presented affected rankings. The survey is available as Supplementary Figure S1 online. The UW Institutional Review Board approved the study (UW IRB Biomedical Committee B, 41829).
UNC researchers with experience in social science and ethnographic research and clinical genetic counseling developed all UNC focus group materials. The final materials consisted of (i) a moderator guide, (ii) a 13-item questionnaire (8 demographic items and 5 genetic testing experience items), (iii) a one-page handout providing an overview of exome sequencing and diagnostic versus incidental information, and (iv) a one-page handout with a vignette describing the exome diagnostic testing experience of a hypothetical patient with a neuromuscular condition. The format for the moderator guide was based on a traditional funneling approach that guides discussion from broad to more specific questions.14,15 This format was used to enable incorporation of new knowledge and to allow opinion formation about exome sequencing and the possibility of findings not related to the diagnostic indication. The informational handout was based on NCGENES education materials. It describes incidental information as genetic results “completely unrelated to the person’s symptoms.” The moderator guide further clarified these results as “any findings that are not related to the reason for ordering the test.” This language is similar to the description of incidental information provided in the UW surveys, although it should be noted that the concept was not described identically to both participant groups. Possible categories of these findings were described to participants to potentially include diagnostic results for a different medical condition (with subcategories of varying severity and ability to treat or prevent), carrier status and statistical associations for pharmacogenetics interactions, and risks for common diseases. The study was approved by the UNC IRB (UNC protocol 13–3466). The development of focus group materials was not informed by the contents or results of the UW survey and vice versa.
Population
Adults who presented for medical genetics evaluation at UW were recruited to the survey study in one of two ways: they were already enrolled in the UW NEXT Medicine study or they were registered patients being examined at the UW Genetic Medicine clinic. All NEXT Medicine participants had consented to be contacted regarding additional study-related activities and were e-mailed a link to the electronic survey. The concept of incidental findings had been introduced by study personnel and in materials during informed consent as “genetic information (results) that may include risks for ‘extra’ diseases other than CRCP.” Those randomized to the exome sequencing arm had also been asked to complete a document eliciting preferences for types of incidental findings; subsequently, those findings were returned. The UW Genetic Medicine clinic patients not in the NEXT Medicine study being seen for a variety of indications could leave their completed paper survey in a collection box at the end of their clinic visit or use a prepaid envelope to return it by mail. Surveys were not given to patients being evaluated for neurocognitive decline or neurodevelopment disorders such as autism.
UNC focus group participants were adult patients or the parents of pediatric or intellectually disabled adult patients who had been evaluated through a UNC Genetics Clinic appointment (pediatric, adult, or cancer) within the previous 2 years. To be eligible, genetic testing had to have been conducted as part of their (or their child’s) evaluation, patients had to be comfortable participating in the focus group discussion in English, and patients had to live within approximately 30–40 min of driving time of the focus group location near UNC Hospitals. An introduction letter was mailed to eligible individuals and follow-up phone calls were used to recruit potential participants who had not opted out.
Implementation
Electronic surveys were e-mailed to 75 UW NEXT Medicine study participants in July 2015 (37 in the usual care group and 38 in the exome sequencing group); they were given 2 weeks to respond. A reminder e-mail was sent to those who had yet to respond 1 week before the end of the survey time period. Paper surveys were distributed to UW Genetic Medicine clinic patients not already enrolled in the NEXT Medicine study during the check-in and intake process of their clinic visit. Responses were collected during 6 clinic days over a period of 5 weeks between 25 June 2015 and 30 July 2015.
Six UNC focus groups were conducted during the autumn of 2013. Each session lasted approximately 2 hours, dinner was provided, and participants received $40. Each focus group contained 3–12 participants who were grouped according to whether they were an adult patient (four groups: two hereditary cancer, one general genetics, and one mixed) or the parent/guardian of a patient (two groups). The first session served as a pilot, and minor modifications were subsequently made to the Moderator Guide. An experienced focus group moderator (J.M.O.) led all sessions. At least one additional research team member was present at each session to take notes. Sessions were audio-recorded and transcribed.
Analyses
Descriptive statistics were compiled for survey responses from UW NEXT Medicine participants and UW Genetic Medicine clinic patients. Fisher’s exact tests were used to evaluate whether sex, age group, race, or population (NEXT Medicine versus clinic) affected respondents’ first-choice term and how strongly they felt that there is a better or worse term. Tests were not corrected for multiple contrasts because they were descriptive.
Consistency across UNC focus groups was supported by using the same researcher to conduct each session following an established moderator guide. Verbatim transcripts of focus groups were analyzed using an iterative process for content analysis.14,16 Each transcript was read independently for context and discussed as a group along with the session notes. A procedure for analysis was developed with agreement from all members of the UNC research team. Transcripts were redistributed and read a second time to group (unitize) relevant themes based on specific moderator guide prompts. Themes were discussed and refined through group discussion. After a consensus was reached on the definition of each theme, a third read of transcripts was conducted, at which time the themes were applied (coded) and exemplar quotes were identified. Descriptive statistics were utilized for responses to the demographic and genetic experience survey.
Results
Demographics and response rate
Of the 88 UW survey respondents (57 NEXT Medicine study participants and 31 Genetic Medicine clinic patients), complete data on terminology preferences were available for 73. One of the 31 UW clinic patients did not select any of the choices, and 10 of the 31 only selected their first choice. Additionally, 7 of the 57 UW NEXT Medicine study respondents provided two rankings for the same term. For consistency, the lowest ranking for each duplicated term was omitted. Thus, the total number of respondents with first-choice rankings was 87. Seventy-seven participants made second- and third-choice rankings, and 73 participants ranked all four terms. Among the 57 UW NEXT Medicine study respondents, significantly more from the exome sequencing group (87%) than from the usual care group (65%) responded (chi-square 4.96; P = 0.026). Survey respondents’ demographic characteristics are listed in Table 1 . There was relatively equal representation of both sexes (47% males and 53% females). The majority of respondents (73/88) identified as white. Additionally, the majority (88%) of the respondents were between 30 and 70 years old.
A total of 40 individuals participated in one of the six UNC focus groups and 37 completed the questionnaire ( Table 2 ). Participants were predominantly female (73%), white (73%), had a college degree (64.9%), and had health insurance (89.2%). Of the nine parents of pediatric or intellectually disabled adult patients who participated, the mean age of their children was 18 years (SD, 9.86; range, 6–35). Although all were known to have had at least one genetic test, five (13.5%) indicated they had never undergone genetic testing or were unsure. In addition, 32.4% did not indicate they understood the meaning of the genetic testing. Most (75.7%) had not heard about exome sequencing prior to the focus group.
Terminology preferences
The ranking of terms from the UW survey is presented in Figure 1 . Among first-choice rankings, nearly two-thirds chose additional findings (51/87) as the overall first choice. One-fifth (17/87) chose secondary findings as their first choice; 13% chose incidental findings and 9% chose ancillary findings. There was no significant difference in first-choice responses between participants in the UW NEXT Medicine study who responded to the electronic survey and UW Genetic Medicine clinic patients who used the paper survey (Fisher’s exact P = 0.09). There was also no difference in survey responses based on race, sex, or age group. Two participants provided comments explaining the reasoning behind their choices. One said, “We did not like the “incidental” findings choice because it conveyed a sense of unimportance where it may, in fact, be very important to the patient.” The other respondent included a comment about each term: (i) secondary findings—“I like this one the best because I feel like it is very specific in describing the findings relative to the primary work”; (ii) ancillary findings—“this one draws a connection between the primary and “secondary” findings”; (iii) additional findings—“implies that there is some connection between the findings”; and (iv) incidental findings—“demotes the importance of the findings, whereas they might in fact be important.”

Rankings of terms sorted by percentage of participants in each survey group (paper versus electronic). The darker blue represents the choices made by participants responding to the paper survey; the lighter blue represents choices made by participants responding to the electronic survey.
Survey respondents were also given the option to suggest a different term. The term unrelated genetic findings was listed twice—once by a NEXT Medicine study participant and once by a UW Genetic Medicine clinic patient. The term supplemental findings was listed three times by UW NEXT Medicine study participants. Other terms suggested only once include secondary/tertiary, subsidiary, unanticipated, further, and collateral findings. Some participants suggested modification of the term additional, such as additional genetic findings and significant additional findings.
When UNC focus group participants were asked to reflect specifically on the term incidental finding, most participants preferred a more neutral term.
“The word ‘incidental’ sounds trivial when you’re talking about ALS or, you know, Alzheimer’s or something... I think that incidental is ‘Am I going to pass on green eyes?’ Much more than ‘Am I going to pass on ALS?’”
“I would prefer a different category, one that implies something that may be meaningful or may need further follow-up or something…”
“If it’s incidental to you, it may not be to me.”
Tasked with suggesting a better term, five of the six groups settled on the term additional; the other group felt that the term incidental was fine to use as long as the clinician explained what was intended.
“‘ Additional’—that way it doesn’t seem threatening”
“I like that, ‘additional findings,’ cause that’s something I’m more familiar with that term. And so, and I would take that—doesn’t mean that’s negative or positive. It’s just this is what has shown up.”
“I find myself wishing I had a thesaurus for looking up other words.”
Survey participant interest level
In the UW study, participants were asked to rate on a scale of 1 to 5 how strongly they felt that some terms were better than others, with 1 indicating “It does not matter to me” and 5 “I feel some are better.” Of the 88 participants, the numbers who chose scores 1–5, respectively, were 25 (28%), 9 (10%), 20 (23%), 13 (15%), and 20 (23%); one person did not respond. These ratings did not differ based on race and sex of respondents; however, marginally more participants in the 18–50 age group than in the >50 group reported that it did not matter (Fisher’s exact test P = 0.052). More participants in the UW Genetic Medicine clinic patients group than in the UW NEXT Medicine study group also reported that it did not matter (Fisher’s exact test P = 0.048, respectively).
Discussion
Incidental findings was the original term used by the scientific community2,17,18,19,20,21,22,23 to describe findings identified from genomic tests that are not related to the indication for testing. The term secondary findings—one of the numerous alternative terms that has been proposed3—was recently endorsed by the ACMG because it was deemed to describe the intentional process of analysis better than other terms.24 The term ancillary findings has also been used by radiology and imaging specialties.5,6,25,26,27 Yet, UW survey and UNC focus group patients participating in our study not only did not prefer any of these terms but also were strikingly consistent in preferring the term additional findings. That is, given an option of four terms, 59% of UW survey respondents ranked the term additional findings above the other terms. Only one-third of survey respondents preferred the term secondary findings. Similarly, UNC focus group participants both volunteered and reached a consensus on additional findings as their preferred term. Thus, our findings reveal discordance between the term typically used by the genetics community and by patients’ preferences from both survey data and open-ended discussion.
This finding may indicate that patients and research participants prefer more familiar words. The words additional and secondary, but not incidental, are listed in the Oxford 3000 (http://www.oxfordlearnersdictionaries.com/us/about/oxford3000), a list of 3,000 of the “most important words to learn in English” based on the criteria of frequency in English across varying types of texts and/or a high degree of familiarity to most English users. UNC focus group participants also preferred a term that was a familiar word.
However, participants also had other reasons for their preferences—they felt the alternative words had connotations that were misleading or inaccurate. Explanations that UN survey respondents offered for their choice included the concern that the term incidental conveys a sense of unimportance. Likewise, UNC focus group participants pointed out that incidental results could be diagnostic of a serious health condition, underscoring their perceived importance. Consequently, these participants suggested using a broader, neutral term that could encompass a range of information. Echoing this sentiment, Dorschner et al.10 criticized the term secondary findings because it may lead to these findings being interpreted as less important than primary findings.
Clearly, patients and providers may understand terms to mean different things, offering another potential explanation for why the preferences of patients and geneticists are discordant. For instance, one justification for using the term incidental findings is that it exists as a medical term with a clear meaning to providers; however, this meaning does not appear to be shared by patients. Medically, the term secondary is used to mean due to another cause or disease, as exemplified by the disorder secondary amenorrhea. It is likely that the participants are not concerned with or aware of the medical usage of the term secondary.
In addition, our findings suggest that greater exposure to the concept of incidental findings may affect the extent to which patients perceived it to be important to use terminology they deemed to be accurate. Specifically, compared to UW Genetic Medicine Clinic patients, a greater proportion of UW NEXT Medicine study participants indicated that they felt some terms were better than others. NEXT Medicine participants discussed the concept of incidental findings several times as part of the study protocol and consented to be part of a trial in which exploring incidental findings was a primary aim; thus, they were likely to have spent more time thinking about the concept of incidental findings as it is currently used in medical genetics practice.
Several limitations should be noted with respect to these findings. Both the UW survey and UNC focus group studies included a relatively small number of participants, the majority of which were white and highly educated, and both studies were conducted at large academic medical centers; therefore, these results may not be generalizable to other settings. Repeating the surveys and focus groups in a more diverse population would increase the generalizability of these results. In addition, the order of alternative terms was not randomized in the paper survey given to UW Genetic Medicine clinic patients. However, our findings suggested that the order in which the terms were listed did not affect patient preferences. Additional findings was listed as the third choice on the paper survey but was the first choice of most. Furthermore, the terms were presented in a random order in the electronic survey and there was no difference in first-choice response between the two groups.
As genomic sequencing technology becomes more integrated into health care, ensuring the use of standard terminology that is meaningful to patients may improve care. The gap between the terminology used by providers and what makes the most intuitive sense to patients may influence the effectiveness of communication. Using language and terms that are familiar and accessible to patients should help ensure that patients are well informed about the various options regarding results available from clinical sequencing laboratories. Facilitating patients’ understanding and their ability to make informed choices should also empower them to actively consider their options concerning additional findings as they decide whether to pursue genomic sequencing (e.g., when considering whether to opt out of interpreting the ACMG 56 medically actionable genes on exome sequencing tests2).
In summary, despite widespread use of the terms incidental findings and secondary findings in medical genetics to describe sequencing results unrelated to the indication for testing, patients appear to prefer the more neutral and accessible term additional findings. Patient perceptions and comprehension will be framed by the terms used. As such, medical genetics professionals should consider this preference when choosing terms to use as they communicate with patients and participants about these findings in the genetics clinic and in research studies.
Disclosure
The authors declare no conflict of interest.
References
Katzman GL, Dagher AP, Patronas NJ. Incidental findings on brain magnetic resonance imaging from 1000 asymptomatic volunteers. JAMA 1999;282:36–39.
Green RC, Berg JS, Grody WW, et al.; American College of Medical Genetics and Genomics. ACMG recommendations for reporting of incidental findings in clinical exome and genome sequencing. Genet Med 2013;15:565–574.
Christenhusz GM, Devriendt K, Dierickx K. Secondary variants–in defense of a more fitting term in the incidental findings debate. Eur J Hum Genet 2013;21:1331–1334.
van El CG, Cornel MC, Borry P, et al.; ESHG Public and Professional Policy Committee. Whole-genome sequencing in health care. Recommendations of the European Society of Human Genetics. Eur J Hum Genet 2013;21 Suppl 1:S1–S5.
Haga SB, Tindall G, O’Daniel JM. Professional perspectives about pharmacogenetic testing and managing ancillary findings. Genet Test Mol Biomarkers 2012;16:21–24.
Haga SB, Tindall G, O’Daniel JM. Public perspectives about pharmacogenetic testing and managing ancillary findings. Genet Test Mol Biomarkers 2012;16:193–197.
Wright CF, Middleton A, Burton H, et al. Policy challenges of clinical genome sequencing. BMJ 2013;347:f6845.
Christenhusz GM, Devriendt K, Peeters H, Van Esch H, Dierickx K. The communication of secondary variants: interviews with parents whose children have undergone array-CGH testing. Clin Genet 2014;86:207–216.
Lyon G. There is nothing ‘incidental’ about unrelated findings. Personalized Medicine 2012;9:163–166.
Dorschner MO, Amendola LM, Turner EH, et al.; National Heart, Lung, and Blood Institute Grand Opportunity Exome Sequencing Project. Actionable, pathogenic incidental findings in 1,000 participants’ exomes. Am J Hum Genet 2013;93:631–640.
Roche MI, Berg JS. Incidental Findings with Genomic Testing: Implications for Genetic Counseling Practice. Curr Genet Med Rep 2015;3:166–176.
Clinical Sequencing Exploratory Research. https://cser-consortium.org/. Accessed 1 December 2016.
Gallego CJ, Bennette CS, Heagerty P, et al. Comparative effectiveness of next generation genomic sequencing for disease diagnosis: design of a randomized controlled trial in patients with colorectal cancer/polyposis syndromes. Contemp Clin Trials 2014;39:1–8.
Stewart DW, Shamdasani PN. Focus Groups: Theory and Practice. Sage Publications: Newbury Park, CA, 1990.
Krueger RA, Casey MA. Focus Groups: A Practical Guide for Applied Research. 3rd edn.Sage Publications: Thousand Oaks, CA, 2000.
White MD, Marsh EE. Content analysis: a flexible methodology. Librar Trends 2006;55:22–45.
Appelbaum PS, Parens E, Waldman CR, et al. Models of consent to return of incidental findings in genomic research. Hastings Cent Rep 2014;44:22–32.
Kleiderman E, Knoppers BM, Fernandez CV, et al. Returning incidental findings from genetic research to children: views of parents of children affected by rare diseases. J Med Ethics 2014;40:691–696.
Shkedi-Rafid S, Dheensa S, Crawford G, Fenwick A, Lucassen A. Defining and managing incidental findings in genetic and genomic practice. J Med Genet 2014;51:715–723.
Turbitt E, Wiest MM, Halliday JL, Amor DJ, Metcalfe SA. Availability of treatment drives decisions of genetic health professionals about disclosure of incidental findings. Eur J Hum Genet 2014;22:1225–1228.
Regier DA, Peacock SJ, Pataky R, et al. Societal preferences for the return of incidental findings from clinical genomic sequencing: a discrete-choice experiment. CMAJ 2015;187:E190–E197.
Ding LE, Burnett L, Chesher D. The impact of reporting incidental findings from exome and whole-genome sequencing: predicted frequencies based on modeling. Genet Med 2015;17:197–204.
Parker LS. The future of incidental findings: should they be viewed as benefits? J Law Med Ethics 2008;36:341–51, 213.
ACMG. ACMG Releases Member Survey Results on Secondary Findings and Reinforces Earlier Recommendations in New Policy Statement on Secondary Findings. 13 November 2014. https://www.acmg.net/docs/Survey_Results_Secondary_findings.pdf. Accessed 22 December 2015.
Begic A, Opankovic E, Cukic V, Lindqvist A, Miniati M, Bajc M. Ancillary findings assessed by ventilation/perfusion tomography. Impact and clinical outcome in patients with suspected pulmonary embolism. Nuklearmedizin 2015;54:223–230.
Wong YC, Wu CH, Wang LJ, Chen HW, Lin BC, Huang CC. Mesenteric vascular occlusion: comparison of ancillary CT findings between arterial and venous occlusions and independent CT findings suggesting life-threatening events. Korean J Radiol 2013;14:38–44.
Stein PD, Matta F, Sedrick JA, Saleh T, Badshah A, Denier JE. Ancillary findings on CT pulmonary angiograms and abnormalities on chest radiographs in patients in whom pulmonary embolism was excluded. Clin Appl Thromb Hemost 2012;18:201–205.
Acknowledgements
We thank all the respondents, the staff of the Center on Human Development and Disability, and the NEXT Medicine Return of Results Committee. The UW NEXT Medicine study was supported by NHGRI and NCI grants U01 HG006507 and U01 H007307. The UNC NCGENES study was supported by UO1 HG006487 and U01 H007307. N.T. (UW) was supported by the American College of Medical Genetics Foundation Summer Scholars Program.
Author information
Authors and Affiliations
Corresponding author
Supplementary information
Supplementary Figure S1
(PDF 326 kb)
Rights and permissions
About this article

Cite this article
Tan, N., Amendola, L., O’Daniel, J. et al. Is “incidental finding” the best term?: a study of patients’ preferences. Genet Med 19, 176–181 (2017). https://doi.org/10.1038/gim.2016.96
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/gim.2016.96
Keywords
This article is cited by
-
The impact of unsolicited findings in clinical exome sequencing, a qualitative interview study
European Journal of Human Genetics (2021)
-
Incidental findings from cancer next generation sequencing panels
npj Genomic Medicine (2021)
-
Whole genome sequencing reveals that genetic conditions are frequent in intensively ill children
Intensive Care Medicine (2019)
-
Meeting report of the 2017 KidGen Renal Genetics Symposium
Human Genomics (2018)
-
Attitudes of stakeholders in psychiatry towards the inclusion of children in genomic research
Human Genomics (2018)
