
Abstract
Purpose To describe referral guidelines for hereditary breast and ovarian cancer (HBOC) counseling among a group of Health Maintenance Organizations (HMOs) and awareness of such among primary care clinicians.
Methods An organizational assessment of plan policies and a primary care clinician survey.
Results Five of the 7 HMOs reported having HBOC referral guidelines. Differences between plan's criteria included age of breast cancer onset, inclusion of male breast cancer, and second-degree relatives. Of the 91% clinicians responding, only half were aware of the HBOC guidelines. Awareness was higher in the plan with the most intense implementation effort (OR = 3.0, 1.5–5.9) and among gynecologists (OR = 2.8, 1.5–5.4).
Conclusions Although HBOC counseling guidelines within participating HMOs identify persons for referral that can be easily incorporated into routine practice, continued work is needed to better understand how to help primary care providers identify high-risk persons, and new models of providing genetic services may need to be considered.
Similar content being viewed by others

Main
In the mid-1990s germline mutations in the BRCA1 and BRCA2 (BRCA1/2) genes were found to be associated with an increased risk for breast and ovarian cancers. 1–2 Genetic testing of the general population for BRCA1/2 mutations is not endorsed, however, because the prevalence is low and the psychosocial consequences are potentially high. 3–12 Rather, the current recommendation by professional organizations is to screen the general population at the primary care level to identify those at potentially increased risk for hereditary susceptibility to breast and ovarian cancer. 3–8,13 Formal genetic counseling and testing would then only be offered to those at the highest level of familial risk.
Primary care providers thus have an important role in identifying patients at increased risk for hereditary susceptibility to breast and ovarian cancer. Studies have confirmed that such providers need and want referral guidance in the emerging area of cancer genetics. 14–17 A number of organizations have published general guidelines to identify patients for whom offering genetic testing is appropriate, and all agree on the importance of genetic counseling by trained professionals as the risks and benefits of testing are complex, personal, and subject to change over time as science and legislation evolve. 3–8
Very little has been published about the use of guidelines in routine primary care to aid in identifying patients for breast and ovarian cancer genetic counseling referral. As the genetics of common diseases expands with new research, the challenge of translation into clinical practice will heighten. A number of Health Maintenance Organizations (HMOs) began offering hereditary breast and ovarian cancer services in the late 1990s, and implemented clinical practice guidelines for referral to such services. 18–19 The purpose of this article is to describe the hereditary breast and ovarian cancer genetic counseling referral guidelines among a group of HMOs in the United States, as well as to explore the awareness of such guidelines among primary care clinicians. The illustration of how selected HMOs have adapted counseling referral guidelines to clinical practice guidelines and the current reported impact of these guidelines among their clinicians can be of value to other organizations and health care providers, particularly those in genetic medicine.
MATERIALS AND METHODS
This analysis is based on data collected as part of DETECT (Detecting Early Tumors Enables Cancer Therapy), a project of the Cancer Research Network (CRN). The CRN is a collaboration of 10 HMOs funded by the National Cancer Institute to increase the effectiveness of preventive, curative, and supportive interventions for major cancers through a program of collaborative research. DETECT is investigating the reasons why women with prepaid access to preventive services would be diagnosed with late-stage breast cancer or invasive cervical cancer. Seven CRN-HMOs participated in DETECT: Group Health Cooperative, Henry Ford Health System, and the Kaiser Permanente Regions in Colorado, Hawaii, Northern California, Northwest, and Southern California.
In 1999, an organizational assessment (OA) gathered data on plan policies and procedures related to breast and cervical cancer screening. Data sources included plan key informant interviews and plan clinical guideline documents on breast cancer screening, cervical cancer screening, and hereditary breast and ovarian cancer susceptibility referral. Details of the data collection and analysis processes have already been described, and included local Institutional Review Board (IRB) approval. 20 Guidelines were submitted by 5 of the 7 plans, with the remaining two plans reporting that no hereditary breast and ovarian cancer susceptibility guidelines for genetic counseling referral existed. For this study, content analysis was performed on the hereditary breast and ovarian cancer susceptibility referral guidelines, an iterative process in which two of the coauthors (J.M., K.V.G.) coded the guidelines into content areas, resolved discrepancies, and then reviewed the findings with each plan's DETECT principal investigator. Content areas included the major risk factors for hereditary breast and ovarian cancer susceptibility, including personal and family history of female breast and ovarian cancers with ages of female breast cancer onset, Ashkenazi Jewish ancestry, and family history of male breast cancer. 8,13 Further content areas included recommendations concerning the provision of genetic and medical management services for hereditary breast and ovarian cancer risk, such as requiring counseling, informed consent, and exclusion of minors, and making medical management recommendations based on testing outcomes.
In 2000, the DETECT project conducted an anonymous survey of primary care clinicians within 3 of the 7 HMOs, each of which obtained IRB approval. The methodology has been described elsewhere. 21 The clinician survey was designed to evaluate clinician demographics, knowledge, attitudes, and beliefs, as well as organizational characteristics affecting adoption and implementation of breast and cervical cancer screening guidelines. Eligible clinicians were physicians, nurse practitioners, and physician assistants within the departments of family medicine, internal medicine, and gynecology, who were in the plan for at least one year and who were involved in patient care at least half-time. All eligible clinicians in two plans and a random sample of clinicians in the third plan were surveyed. A four-stage data collection process consisting of a mailing, a follow-up mailing, a reminder telephone call or e-mail from a local leader involved in the project, and a telephone call from a professional survey organization was used to maximize response rates.
The survey included one question on provider awareness of plan referral guidelines for hereditary breast and ovarian cancer susceptibility. In the bivariate and multivariate analyses, a “correct” answer for awareness of the hereditary breast and ovarian cancer susceptibility guidelines was based on the organizational assessment data. That is, we created a correct awareness variable by cross-classifying each clinician's self-reported awareness of guidelines with the actual plan guidelines collected during the organizational assessment. Thus, clinician's reporting awareness of a truly existing guideline had “correct” awareness of that guideline.
We hypothesized that awareness of the hereditary breast and ovarian cancer susceptibility guideline might be associated with the reported rating of usefulness for the general breast cancer screening guideline. Using a 5-point scale, respondents were asked about general breast cancer screening, including asking respondents to rate the overall usefulness of their plan's breast cancer screening guideline to their practice. It is important to note that this item referred to the plan's breast cancer screening guideline, not the hereditary breast and ovarian cancer susceptibility guideline, and that this item was located in the general breast cancer screening section of the survey. Logistic regression was performed with the dependent variable being correct knowledge of existence of hereditary breast and ovarian cancer susceptibility referral guidelines, again as determined from the organizational assessment data.
RESULTS
Guideline Content
Table 1 reports the content and criteria of the guidelines from the five plans. Four of the five plans' hereditary breast and ovarian cancer susceptibility guidelines relate to genetic counseling referral only and the remaining plan's guideline is a combination of referral and testing. All of these plans' hereditary breast and ovarian cancer susceptibility guidelines were initially implemented in 1997, although the guideline that was current in 1999–2000 varied in the year of development from 1997–1999. The five plans each have plan-specified policies requiring revisiting and, if applicable, revising the content of the guideline. Thus, the guidelines reported here are not static documents. All the guidelines include text, describing the background of the material and the sources of evidence, as well as tables, flow charts, or bulleted lists indicating patients to consider for referral.
The guidelines all include criteria for counseling/testing referral, with the criteria based on well-delineated personal cancer history factors (breast and ovarian), family cancer history factors (breast and ovarian), and combined personal and family cancer history, as well as family history of a known mutation. As shown in Table 1, there is consistency across the guidelines, yet there is also variation. For the four plans with referral guidelines, the age of breast cancer onset in a woman of Ashkenazi Jewish descent varies with ≤ 40 years of age at three plans, and ≤ 45 years of age at one plan. Two plans do not include male breast cancer in the pedigree within their illustrated indicators for referral. However, both of these plans include discussion of male breast cancer and increased BRCA1/2 mutation risk in the text of their guidelines. The plan with referral and testing guidelines does not include the cancer history of second-degree relatives as a referral or testing criteria among unaffected persons.
In addition to providing criteria for counseling referral, all of the guidelines also include recommendations. All but one plan's guidelines include specific language about requiring pretest genetic counseling. This plan's guideline, however, is written for the purpose of identifying persons appropriate for genetic counseling referral. Informed consent before testing is required within all of the collected guidelines, with indication that persons referred must have the mental competence to provide such written informed consent. Each of the four plans with referral-only guidelines address the appropriateness of referring persons who do not meet criteria but have significant anxiety. These four plans' guidelines also include specific language for unacceptable referrals, such as for minors. Although variable in detail, four plans' referral guidelines further include medical management options for individuals who are tested and found to have a mutation in the BRCA1/2 genes. Two plans have language to recommend that an affected relative be tested first.
Clinician awareness of guidelines
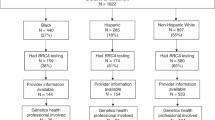
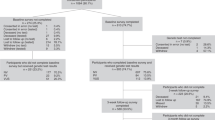
Three of the HMOs with hereditary breast and ovarian cancer susceptibility referral guidelines also participated in the clinician survey. Overall, the clinician survey had a 91% response rate (N = 621) with plans' response rates varying from 83% to 100%. Of the returned surveys, N = 612 responded to the awareness of hereditary breast and ovarian cancer susceptibility guideline question and thus were eligible for analyses. Clinician characteristics are reported in Table 2. Family medicine specialty was reported by 45%, with a nearly even split between females and males. The majority of respondents were physicians (74%), 70% reported birth dates in the 1950s or later, and 34% reported employment within the HMO between 11 and 20 years.
Fifty-two percent of respondents reported awareness of these guidelines (Table 3). Awareness was highest at plan B, and among gynecologists at all plans (both values P < 0.001). Awareness of hereditary breast and ovarian cancer susceptibility guidelines was also higher among physicians and nurse practitioners than among physician assistants (P = 0.005) and was associated with more than five years of employment within the organization (P = 0.02). Awareness of the hereditary breast and ovarian cancer susceptibility guidelines was greater among providers reporting higher clinical usefulness of the general breast cancer screening guidelines at their organizations (P < 0.0001). Logistic regression was performed with the final model making adjustment for plan, medical specialty, medical discipline, age, numbers of years with HMO, and reported usefulness of the general breast cancer screening guidelines. Gender did not contribute significantly to the final model, nor did possible interactions. The adjusted odds of hereditary breast and ovarian cancer guideline awareness were significantly greater in plan B (OR = 3.0, 1.5–5.9), among gynecologists (OR = 2.8, 1.5–5.4), and among providers reporting a very high clinical usefulness of plan breast cancer screening guidelines (OR = 2.6, 1.7–3.8).
DISCUSSION
This study found that 5 of 7 HMOs participating in the DETECT project have hereditary breast and ovarian cancer susceptibility clinical practice genetic counseling referral guidelines relevant to routine primary care practice. Of the remaining two plans, both offer and cover the costs of hereditary breast and ovarian cancer susceptibility counseling and testing, but neither have referral guidelines in place to identify high-risk patients for such services.
Nearly all of the HMOs that reported hereditary breast and ovarian cancer susceptibility referral guidelines for this project have detailed outlines identifying persons for referral based upon evidence available at the time of guideline development (1997–1999). Among these five plans' guidelines, only two points vary noticeably. First, one plan does not include affected second-degree relatives in identifying criteria for referral among unaffected persons. It is important for referring providers to understand that mutations in the BRCA1/2 genes can be transmitted through the paternal lineage, and therefore, cancer history from second-degree relatives within the paternal side is particularly important in referral guidelines. Further, for both maternal and paternal lineages, second-degree family history is important, as these genetic mutations are not fully penetrant. 13 Secondly, two plans do not address male breast cancer in the pedigree as a criterion for referral in the guideline figures, but such is included in the text. Although providers can still refer such persons, it is important to include this indicator as a visual diagram in addition to the text so it is not inadvertently overlooked by busy clinicians. Both of these issues indicate the need for input from clinical genetics during future guideline development.
Although the majority of these HMOs' guidelines were for genetic counseling referral, rather than testing, one testing issue with referral implications was also evident. Only two plans' guidelines recommend that an affected relative be tested before any unaffected persons if possible. Without testing an affected relative first, a negative BRCA1/2 result can have different interpretations with very different disease risk assessments, with clarity coming only from testing an affected family member. It is possible that some plans did not feel this was needed in a referral guideline, because which family member to be tested first is a decision made after review of a complete pedigree. It is vital, however, for referring providers to understand that another family member may need to be referred in addition to the initial referral. Although testing the family member with the greatest pretest probability may be preferred, in practice this can be difficult. However, as more insurers begin to cover the costs of genetic counseling and testing, it may be necessary for ensuring high quality care that insurance carriers agree to cover the costs of genetic counseling and testing for their respective membership, even if the test would provide the most direct medical benefit for a nonmember. Guideline committees and benefit committees will be challenged when creating future versions of cancer genetic counseling referral guidelines about how to address referral and coverage of nonmembers, and providers of genetic medicine may need to be advocates in these processes.
Only half of clinicians surveyed at these plans were aware of plan referral guidelines for hereditary breast and ovarian cancer susceptibility. Hereditary predisposition for cancer accounts for only a small portion of all cancer, yet genetic services identifying hereditary breast and ovarian cancer susceptibility may be important in reducing cancer morbidity and mortality, as risk reduction efforts could be targeted to those identified with high hereditary cancer risk. 22–24 Further, such services could allow reassurance for women who are not at high risk for an inherited predisposition to breast or ovarian cancers, and may additionally allow patients a level of informed choice that may not be achievable in daily primary care. Indeed, previous literature suggests that primary care providers are not well-informed to discuss the issues of cancer genetics with patients. 14–17 Further, studies suggest that in general women are not well-informed regarding inherited risk for cancer and that they seek information from their family members rather than their health care providers. 25–26
A referral guideline to help primary care providers identify which members are at increased risk for inherited susceptibility for breast and ovarian cancers would thus seem to be a potential solution to this problem. Indeed, most of the HMOs that participated in this study have such referral guidelines, as well as a long history of cancer prevention guidelines, methods to promulgate those guidelines, and system levels of implementing many of the guidelines. 20 That gynecologists reported significantly greater awareness than other specialties is supported by previous studies that show the majority of BRCA1/2 testing referrals come from gynecologists. 16 That awareness was associated with plan may be explained by the level of implementation effort, which clearly was associated with provider awareness at these three plans. For example, Plan B's implementation included not only dissemination of the guidelines, but also dissemination of educational materials for physicians, including articles on breast cancer and genetic risk in physician-directed magazines, interactive videoconferencing, and training seminars for physicians. Plan E's implementation effort was posting of the guideline on a well-used internal web page that helped providers sort through who was really at high risk for breast cancer, and well-publicized description of what services were available to the primary care provider. Plan D's implementation was a written guideline that was distributed with other preventive service guidelines, and annual presentation of the preventive services' guidelines at primary care department meetings.
Despite such plan efforts, however, overall our work suggests that even within these HMOs, referral guideline development and implementation for breast and ovarian cancer genetic services may not be enough to assure awareness and use by clinicians. Educating primary care providers would likely only have a limited lasting effect based on the literature on changing physician behavior and because cancer genetic services are not an issue for the majority of primary care patients. 27–29 Thus, perhaps to best incorporate cancer genetics into medicine, a more system-wide approach or outreach implementation is needed, such as what has been put in place at many HMOs for general breast and cervical cancer. 20 For such a new model of genetic risk identification to work, however, those trained in genetic medicine will need to be key players not only in establishing the systems for identification of risk and triage but also in continuing to oversee the translation of new findings into such clinical practice.
One limitation of this work is that the DETECT HMOs are not a representative sample of managed care organizations. Data collection was only conducted on the group or staff model component of these HMOs. However, for study of hereditary breast and ovarian cancer susceptibility referral guidelines, it was important to explore HMOs with a history of provision of preventive services and a history of effective plan guideline adoption and implementation for preventive services. We acknowledge that five of the participating plans are Kaiser Permanente regions formed by exclusive Permanente Medical Group contracts with the Kaiser Foundation Health Plan. Activities undertaken in these organizations may be more interdependent than those of the two non-Kaiser Permanente plans.
The organizational assessment was cross-sectional in design, and as such, may not represent current guideline content. The clinician survey was also cross-sectional and limited by the small number of participating plans, however, our results are strengthened by the markedly high response rate. We acknowledge that outcome measures such as numbers of and criteria of actual referrals to hereditary cancer services were not collected on the clinician survey. Although awareness of the guidelines is important, it is possible that providers are aware of cancer genetic referral services without being aware of the plan's clinical practice referral guidelines. As such, the percentage of actual referrals that comply with the plans' referral guidelines may not vary across the three HMOs regardless of provider awareness. We doubt that this is true, however, because among these three HMOs the use of plan guidelines for other cancer prevention services is high while the number of referrals for breast and ovarian cancer genetic services during the time period was low. Although across plans the percentages of guideline awareness were lower than was hypothesized, without further data it is difficult to validly interpret the clinical impact of the reported level of awareness. Yet we are confident to conclude that to achieve maximal effect on cancer prevention, continued work needs to be done including potentially new models of providing cancer genetic services in order to learn how best to increase the awareness and use of this information by primary care clinicians.
References
Miki Y, Swensen J, Shattuck-Eidens D, Futreal PA, Harshman K, Tavtigian S A strong candidate for the breast and ovarian cancer susceptibility gene BRCA1. Science 1994; 266: 120–122.
Wooster R, Neuhausen SL, Mangion J, Quirk Y, Ford D, Collins N Localization of a breast cancer susceptibility gene, BRCA2, to chromosome 13q12-13. Science 1994; 285: 2088–2090.
Statement of the American Society of Hum Genet on genetic testing for breast and ovarian cancer predisposition. Am J Hum Genet 1994; 55: i–iv. Available at: http://www.ash.org/genetics/ashg/pubs/policy/pol-11.htm. Accessed September 30, 2003.
Committee on genetics. ACOG committee opinion breast-ovarian cancer screening. Int J Gynecol Obstetrics 1997; 56: 82–83.
American Medical Association. Identifying and managing hereditary risk for breast and ovarian cancer. 2003. Available at: http://www.ama-assn.org/ama/pub/category/10183.html. Accessed September 30, 2003.
Statement of the American Society of Clinical Oncology. Genetic testing for cancer susceptibility. J Clin Oncol 1996; 14: 1730–1736.
Hoskins KF, Stopfer JE, Calzone KA, Merajver SD, Rebbeck TR, Garber JE Assessment and counseling for women with a family history of breast cancer: A guide for clinicians. JAMA 1995; 273: 577–585.
American College of Medical Genetics Professional Practice, and Guidelines Committee. Genetic susceptibility to breast and ovarian cancer: Assessment, counseling, and testing guidelines executive summary. 1999: 1–36. Available at: http://www.health.state.ny.us. Accessed September 30, 2003.
Lerman C, Narod S, Schulman K, Hughes C, Gomez-Caminero A, Bonney G BRCA1 testing in families with hereditary breast-ovarian cancer: A prospective study of patient decision making and outcomes. JAMA 1996; 275: 1885–1892.
Lerman C, Croyle R Psychological issues in genetic testing for breast cancer susceptibility. Arch Intern Med 1994; 154: 609–616.
Lodder L, Frets PG, Trijsburg RW, Meijers-Heijboer EJ, Klijn JG, Duivenvoorden HJ Psychological impact of receiving a BRCA1/BRCA2 test result. Am J Med Genet 2001; 98: 15–24.
Meiser B, Butow PN, Barratt AL, Schnieden V, Gattas M, Kirk J, Psychological Impact Collaborative Group. Long-term outcomes of genetic counseling in women at increased risk of developing hereditary breast cancer. Patient Educ Couns 2001; 44: 215–225.
Cummings S, Olopade O Predisposition testing for inherited breast cancer. Oncology 1998; 12: 1227–1241.
Mouchawar J, Klein C, Mullineaux L Colorado physicians' hereditary breast cancer knowledge and practice behavior. J Cancer Educ 2001; 16: 33–37.
National Institutes of Health National Cancer Institute Applied Research Program. National physician survey on genetic testing for inherited cancer susceptibility. Presented at 5th International Symposium on Preventive Oncology and Therapy. Geneva; October 2000.
Acton RT, Burst NM, Casebeer L, Ferguson SM, Greene P, Laird BL Knowledge, attitude, and behaviors of Alabama's primary care physicians regarding cancer genetics. Acad Med 2000; 75: 850–852.
Escher M, Sappino AP Primary care physicians' knowledge and attitudes towards genetic testing for breast-ovarian cancer predisposition. Ann Oncol 2000 11: 1131–1135.
Kutner SE Breast cancer genetics and managed care: The Kaiser Permanente experience. Cancer 1999; 86( suppl 11): 2570–2574.
Myers MF, Doksum T, Holtzman NA Genetic services for common complex disorders: surveys of health maintenance organizations and academic genetic centers. Genet Med 1999; 1: 272–285.
Goins KV, Zapka J, Geiger A, Solberg L, Mouchawar J, Gilbert J, Ulcickas-Yood M, Taplin S Implementation of systems strategies for breast and cervical cancer screening services in Health Maintenance Organizations. Am J Manag Care In press.
Puleo E, Zapka J, White M, Mouchawar J, Somkin C, Taplin S Caffeine, cajoling and other strategies to maximize clinician survey response rates. Eval Health Prof 2002; 25: 169–184.
Malone KE, Daling JR, Thompson JD, O'Brien CA, Francisco LV, Ostrander EA BRCA1 mutations and breast cancer in the general population: analyses in women before age 35 years and in women before age 45 years with first-degree family history. JAMA 1998; 279: 922–929.
Isaacs C, Peshkin BN, Schwartz M, Demarco TA, Main D, Lerman C Breast and ovarian cancer screening practices in healthy women with a strong family history of breast or ovarian cancer. Breast Cancer Res Treat 2002; 71: 103–112.
Scheuer L, Kauff N, Robson M, Kelly B, Barakat R, Satagopan J Outcome of preventive surgery and screening for breast and ovarian cancer in BRCA mutation carriers. J Clin Oncol 2002; 20: 1260–1268.
Velicer CM, Taplin S Genetic testing for breast cancer: where are health care providers in the decision process?. Genet Med 2001; 3: 112–119.
Tessaro I, Borstelmann N, Regan K, Rimer BK, Winer E Genetic testing for susceptibility to breast cancer: findings from women's focus groups. J Womens Health 1997; 6: 317–327.
Davis DA, Thomson MA, Oxman AD, Haynes B Changing physician performance. A systematic review of the effect of continuing medical education strategies. JAMA 1995; 274: 700–705.
Davis D, Thomson O'Brien MA, Freemantle N, Wolf FM, Mazmanian P, Taylor-Vaisey A Impact of formal continuing medical education: Do conferences, workshops, rounds, and other traditional continuing education activities change physician behavior or health care outcomes?. JAMA 1999; 282: 867–874.
Tu K, Davis D Can we alter physician behavior by educational methods? Lessons learned from studies of the management and follow-up of hypertension. J Cont Med Ed Health Prof 2002; 22: 11–22.
Acknowledgements
The project described was supported by Grant Number NIH 5 U19 CA79689 from the National Institutes for Health (Edward Wagner, MD, MPH, Principal Investigator) and its contents are solely the responsibility of the authors and do not necessarily represent the official views of the National Cancer Institute. The Cancer Research Network (CRN) organizations participating in this study consist of the following organizations and principal staff: Group Health Cooperative, Stephen Taplin, MD, MPH (Principal Investigator), Deb Casso, MPH; Kaiser Permanente Northern California, Lisa Herrinton, PhD (Principal Investigator), Michelle Manos, PhD, Carol Somkin, PhD; Kaiser Permanente Colorado, Judy Mouchawar, MD, MSPH (Principal Investigator), Kim Bischoff, MHA; Meyers Primary Care/Fallon, Terry Field, ScD (Principal Investigator), Jane Zapka, ScD, Elaine Puleo, PhD, Mary Jo White, Karin Valentine Goins, MPH; Kaiser Permanente Hawaii, Joyce Gilbert, MPH (Principal Investigator); Kaiser Permanente Southern California Pasadena, CA, Ann M. Geiger, PhD (Principal Investigator); Henry Ford Health System, Marianne UlcickasYood, ScD (Principal Investigator), Sharon Hensley Alford, MPH; Kaiser Permanente Northwest, Sheila Weinmann (Principal Investigator).
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Mouchawar, J., Goins, K., Somkin, C. et al. Guidelines for breast and ovarian cancer genetic counseling referral: Adoption and implementation in HMOs. Genet Med 5, 444–450 (2003). https://doi.org/10.1097/01.GIM.0000093979.08524.86
Received:
Accepted:
Issue Date:
DOI: https://doi.org/10.1097/01.GIM.0000093979.08524.86
Keywords
This article is cited by
-
Use of a Patient‐Entered Family Health History Tool with Decision Support in Primary Care: Impact of Identification of Increased Risk Patients on Genetic Counseling Attendance
Journal of Genetic Counseling (2015)
-
Guidelines for Genetic Risk Assessment of Hereditary Breast and Ovarian Cancer: Early Disagreements and Low Utilization
Journal of General Internal Medicine (2009)
-
Increasing Utilization of Cancer Genetic Counseling Services Using a Patient Navigator Model
Journal of Genetic Counseling (2007)
