
Abstract
Purpose
To evaluate the effect of image compression of spectral-domain optical coherence tomography (OCT) images in the examination of eyes with exudative age-related macular degeneration (AMD).
Methods
Thirty eyes from 30 patients who were diagnosed with exudative AMD were included in this retrospective observational case series. The horizontal OCT scans centered at the center of the fovea were conducted using spectral-domain OCT. The images were exported to Tag Image File Format (TIFF) and 100, 75, 50, 25 and 10% quality of Joint Photographic Experts Group (JPEG) format. OCT images were taken before and after intravitreal ranibizumab injections, and after relapse. The prevalence of subretinal and intraretinal fluids was determined. Differences in choroidal thickness between the TIFF and JPEG images were compared with the intra-observer variability.
Results
The prevalence of subretinal and intraretinal fluids was comparable regardless of the degree of compression. However, the chorio–scleral interface was not clearly identified in many images with a high degree of compression. In images with 25 and 10% quality of JPEG, the difference in choroidal thickness between the TIFF images and the respective JPEG images was significantly greater than the intra-observer variability of the TIFF images (P=0.029 and P=0.024, respectively).
Conclusions
In OCT images of eyes with AMD, 50% of the quality of the JPEG format would be an optimal degree of compression for efficient data storage and transfer without sacrificing image quality.
Similar content being viewed by others

Introduction
The influence of image compression on the quality of the image has been mainly investigated in the field of radiology. Because of the marked increase in the data of medical images owing to the development of new imaging devices in radiology, the proper management of the huge amount of data has been raised as one of the important issues confronting radiology.1, 2 Determining the optimal degree of image compression has been considered as one of the solutions.3, 4 The recent development of high-resolution ocular imaging modalities5, 6 raises the question of how to manage the data more efficiently, and this will be an important issue in the near future, even in the field of ophthalmology.
Spectral-domain optical coherence tomography (SD-OCT) provides high-resolution imaging that allows more detailed retinal and choroidal evaluation.5, 7, 8 However, improvement in the resolution of the images inevitably accompanies the increase in the size of the image. In addition to the problems related to storage of data, the increased size of the image may interfere with prompt patient care based on an electronic medical record system owing to the time delay in exporting the images. The increased size of the data may also be a potential problem when conducting studies using web-based data collection. Thus, some degree of image compression will be necessary for facilitating the handling of a large amount of data.
Although the influence of image compression on the quality of fundus photography has been reported by several investigator groups,9, 10, 11, 12 only a few studies evaluated the influence of image compression on time-domain OCT images (TD-OCT) in healthy eyes.13 The influence of image compression on the interpretation of SD-OCT in eyes with pathologic conditions remains to be elucidated.
Exudative age-related macular degeneration (AMD) is a disorder which needs detailed evaluation of the retinal and choroidal microstructure for the establishment of proper treatment decisions. Previous studies demonstrated that a difference in the resolution of the image between the SD-OCT and the TD-OCT has a significant influence on the detection of retinal pathology associated with disease activity.14, 15, 16
The purpose of the present study was to evaluate the influence of image compression of SD-OCT images on the imaging of eyes with exudative AMD. We additionally attempted to find the optimal degree of image compression for achieving the smallest size of the image without influencing the treatment decision.
Materials and methods
This retrospective observational case series included 30 eyes of 30 patients with exudative AMD. This study was performed at a single center according to the tenets of the Declaration of Helsinki. The study was approved by the institutional review board (IRB No. #2013-03-045).
Patients
We conducted a review of the medical records of patients who were diagnosed with exudative AMD. Images acquired via OCT scanning between January 2011 and January 2012 were analyzed. The diagnosis was made based on the results of 90 diopter lens slit-lamp biomicroscopy, fluorescein angiography, and indocyanine green angiography. Exudative AMD was diagnosed when there was evidence of hyperfluorescence with late leakage associated with pigment epithelial detachment in the macular region, serous retinal detachment, subretinal exudation, and hemorrhage. Only treatment-naïve eyes were included. Additional exclusion criteria included significant media opacity or a thick subfoveal hemorrhage that may preclude acquisition of a clear OCT image.
The horizontal scans centered at the center of the fovea were conducted using SD-OCT (Spectralis, Heidelberg Engineering GmbH, Heidelberg, Germany). Enhanced depth imaging OCT scaning was also performed in the same manner. To improve visualization, 70 to 100 scans were averaged for each section. The images were exported in the uncompressed Tag Image File Format (TIFF) and compressed in the Joint Photographic Experts Group (JPEG) format using the Heidelberg Eye Explorer software (version 1.7.0.0). The JPEG files with 100, 75, 50, 25, and 10% of the quality of JPEG images were exported. Eventually, six images with different formats (one TIFF image and five JPEG images with different degrees of compression) were exported and analyzed for a single OCT image. OCT images were taken before treatment, and after three times of monthly intravitreal ranibizumab injections. In eyes that had a relapse of the disease after treatment, the relapse was confirmed by fluorescein angiography, and OCT images were also taken at the time the relapse was diagnosed.
Outcome measures
Images were displayed on a 22-inch LCD screen with dimensions of 1280 × 1024 pixels, using Image J software (National Institute of Health, Bethesda, MD, USA). The images were magnified to fit the size of the entire screen. The infrared image and scale bar were covered by an independent assistant because in our pilot study the infrared image was found to be easily distorted by image compression.
The images were analyzed in the following order. Firstly, the prevalence of subretinal and intraretinal fluids which may be crucial for determining the activity of the disorder was estimated. Secondly, comparison of the compressed JPEG images with the TIFF images was performed using a dual monitor system, by disguising the image that was compressed. Quality of the compressed images was classified as follows: A: indistinguishable from uncompressed image, B: hardly distinguishable, C: easily distinguishable, but may not influence the treatment decision. D: easily distinguishable, and improvement of the quality of the image will be necessary to establish the appropriate treatment decision. In cases where the graders determined that the quality of the compressed image was better, this image was classified as indistinguishable. After completing the aforementioned two analyses for all the images, the determinability of the subfoveal chorio–scleral interface was estimated using the horizontal enhanced depth imaging OCT images taken before treatment. Classification of the determinability of the subfoveal chorio–scleral interface was as follows: easily determinable, hardly determinable, and undeterminable. Also, subfoveal choroidal thickness was measured for each enhanced depth imaging OCT image using a caliper provided by Image J software. Because a significant overestimation of the subfoveal choroidal thickness was noted when measurement was done using images with a 1 : 1 pixel setting,17 all the measurements were performed using images with a 1 : 1 micron setting. Choroidal thickness of each TIFF image was measured twice by the same examiner (JHK) and the absolute value of the difference between the first and the second measurement was defined as the intra-observer variability in the TIFF image. To evaluate whether the difference in the choroidal thickness measurement between the TIFF and JPEG images was beyond the range of the intra-observer variability of the TIFF image, the absolute value of the difference in choroidal thickness between the TIFF and JPEG images was compared with the intra-observer variability in the TIFF image. Choroidal thickness measurements were conducted in random order with no consecutive measurements for the same image.
Two examiners (JHK and JRK) who were masked to the file format and the degree of compression of images jointly performed the qualitative enhanced depth imaging OCT analysis. The prevalence of intraretinal or subretinal fluid and determinability of the subfoveal chorio–scleral interface were determined by the agreement between the two examiners. The two examiners were masked to the file format and the degree of compression of the images.
The greatest degree of compression that satisfied the following two conditions was selected as the optimal degree of compression: (1) absolutely the same capability to detect subretinal and intraretinal fluids when compared with the TIFF image, and (2) no significant difference between the intra-observer choroidal thickness measurement variability in the TIFF image and difference in choroidal thickness between the TIFF image and compressed image.
Statistics
Statistical analyses were performed with the commercially available software package (SPSS version 18.0 for Windows; SPSS Inc., Chicago, IL, USA). A comparison of the choroidal thickness measurement values between the images with different degrees of compression was performed with repeated measures analysis of variance with Bonferroni’s method. A P-value<0.05 was considered significant.
Results
The mean (± standard deviation) age of 30 patients was 65.4±7.0 years (range 51–84 years), and the mean spherical equivalent was 0.21±1.56 diopters (range −4.5 to +3.5 diopters).
Table 1 summarizes the results of the analyses. In the analyses with the OCT images taken before treatment, the mean size of the TIFF and 100, 75, 50, 25, and 10% of the quality of the JPEG images were 2210 kb (kilobytes), 435.8±40.9 kb, 109.0±16.8 kb, 72.6±11.7 kb, 46.4±7.2 kb, and 25.8±3.1 kb, respectively. The prevalence of subretinal and intraretinal fluids was completely matched among all images regardless of the degree of compression. The majority of the images with 100 or 75% quality of the JPEG images were indistinguishable or hardly distinguishable from the TIFF images. None of the images needed improvement in terms of quality to establish the appropriate treatment decision, despite the quality being easily distinguishable from that of the TIFF image in majority of the JPEG images with 25 and 10% quality (Figure 1). The results were relatively consistent in the analyses with images taken after three times of monthly intravitreal ranibizumab injections. Although the presence of the intraretinal fluid was undeterminable in two (6.6%) images with 10% of quality of the JPEG image, improvement of the quality of the image was not needed to make an appropriate treatment decision. Relapse of the disease was documented in 12 eyes. The results of the analyses in these eyes were almost similar to those with images taken before the treatment. The prevalence of subretinal and intraretinal fluids was perfectly matched among all kinds of images and none of the images needed improvement in terms of quality.

Comparison between an image of the Tag Image File Format (TIFF) format and images of the Joint Photographic Experts Group (JPEG) compression format with various degrees of compression in a treatment-naive eye with exudative age-related macular degeneration. The size of the OCT images were as follows; TIFF=2210 kb, JPEG (75%)=85 kb, JPEG (50%)=56 kb and JPEG (10%)=22 kb. It is notable that intraretinal (arrows) and subretinal fluid (arrowhead) are well-recognized even in the JPEG image of the highest compression rate despite the size of this image being ∼1/100 of the uncompressed TIFF image.
The chorio–scleral interface was well-determined in 73.3% of the images with both TIFF and 100% of the quality of JPEG formats. The proportion was decreased to 60.0%, 53.3%, 36.7%, and 23.3% in compressed images with 75, 50, 25, and 10% of the quality of JPEG, respectively. An undeterminable chorio–scleral interface was noted in 3.3%, 3.3%, 3.3%, 3.3%, 10.0%, and 33.3% of the images among the TIFF images and images with 100, 75, 50, 25, and 10% of the quality of JPEG, respectively. Figure 2 shows the difference in determinability of the chorio–scleral interface between the TIFF and compressed image. The mean choroidal thicknesses measured based on the TIFF and 100, 75, 50, 25, and 10% of the quality of JPEG images were 209.8±86.4 μm, 210.1±86.4 μm, 210.2±86.6 μm, 209.9±84.7 μm, 211.9±87.9 μm, and 212.9±91.8 μm, respectively. In simple comparison, the choroidal thickness measured based on TIFF images was not significantly different from that measured based on JPEG images (P=0.984). The absolute value of intra-observer variability of the choroidal thickness measurement in TIFF images was 8.9±6.2 μm. The absolute value of the difference in choroidal thickness measurement between TIFF and compressed images in images with 100, 75, 50, 25, and 10% of the quality of JPEG was 9.5±4.7 μm, 9.4±7.2 μm, 10.6±7.4 μm, 16.0±11.1 μm, and 18.2±12.3 μm, respectively. The absolute value of the difference in choroidal thickness measurement in JPEG images was significantly different from the intra-observer variability of TIFF images (P=0.022). The difference was not significant in images with 100, 75, and 50% quality of JPEG (P=1.000, P=1.000, and P=1.000, respectively), whereas the difference was significant in images with 25 and 10% quality of JPEG (P=0.029 and P=0.024, respectively).

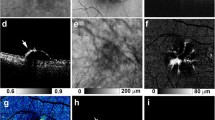
The 1 : 1 micron setting enhanced depth imaging optical coherence tomography images with the Tag Image File Format (TIFF, top) and 50% (middle) and 10% (bottom) quality of Joint Photographic Experts Group (JPEG) compression format in an eye with exudative age-related macular degeneration. The subfoveal chorio–scleral interface, which is relatively well-identified in the TIFF image (top, arrowheads) is undeterminable in the 10% JPEG image (bottom).
Discussion
In the present study, a small amount of subretinal or intraretinal fluid that was observed in the uncompressed TIFF images can be detected in compressed JPEG images of 25% or better quality. However, at least 50% quality of JPEG was necessary for appropriate choroidal evaluation. As a result, compressed images with 50% quality of JPEG was found to be an optimal degree of compression that showed sufficient quality in evaluating both the retina and choroid in exudative AMD. Results of the present study may provide useful information when a clinician used compressed images.
An image with 100% quality of JPEG was almost the same as an uncompressed TIFF image, and the image with 75% of the quality of JPEG was not easily distinguishable from the TIFF image even in the magnified view. The prevalence of subretinal and intraretinal fluids, and subfoveal choroidal thickness was not different between the images with 75 or 100% quality of JPEG and TIFF images. The size of the compressed images with 100 and 75% quality of JPEG was only ∼1/5 and 1/20 of the TIFF images, respectively. Based on this result, it is possible that TIFF images can be substituted by compressed images of better than 75% of the quality of JPEG even for professional usage, such as for medical investigations or making figures for medical journals, as well as for treating patients.
The presence of subretinal and/or intraretinal fluid on an OCT image are signs indicating disease activity in exudative AMD. The presence or absence of these findings on OCT images provides useful information in determining the necessity for treatment.18 We believe that complete agreement between a compressed image and an uncompressed image in detecting these findings will be needed when we attempt to use a compressed image in treating patients because a mistake in determining the amount of fluid accumulation may lead to malpractice. It was notable that images with 25% quality of the JPEG showed complete agreement with the TIFF images in detecting subretinal and intraretinal fluid despite the mean size of images being ∼1/35 to 1/61 of the TIFF images.
However, one weakness of the images with 25% quality of the JPEG was the insufficient quality of deeper tissue images. Approximately 63% of the images showed a hardly determinable or undeterminable subfoveal chorio–scleral interface in images with 25%. The proportion was only 27% in uncompressed TIFF images. Choroidal evaluation is important in the diagnosis and post-treatment follow-up of exudative AMD and allied diseases because polypoidal choroidal vasculopathy usually exhibits a thick choroid,19, 20 whereas typical exudative AMD usually exhibits a thin choroid.19, 20 In addition, a recent study suggested that investigating choroidal morphology as well as estimating choroidal thickness are also important in treating exudative AMD.21 Given this, the uncompressed image may not be substitutable for images with 25% of the quality of JPEG in cases where the quality of the choroidal image is not sufficient.
Eventually, among the five different compression degrees, 50% quality of JPEG was found to be the optimal degree of image compression, achieving the smallest size of image without influencing the treatment decision. The mean size of the compressed images with 50% of the quality of JPEG images was only 1/22 to 1/40 of TIFF images. We believe that using this compressed image will provide more efficient data storage and faster data transmission.
In previous reports that investigated choroidal thickness using exported OCT images, the exact file format and degree of compression were not routinely described. The results of the present study show that using a high degree of image compression may lead to measurement error and this suggests that an uncompressed image or an image with a low degree of compression should be used in medical investigations.
This study has several limitations. First, the analyses were performed for only one of the various commercially available SD-OCT devices. Because the imaging algorithm and size of the raw file could be different among devices, our results may not be valid for other OCT devices. Second, image J software was used as the image viewer in this study. Because different image viewers may have different characteristics, our results may not be valid in some aspects if the clinician uses a different image viewer. Last, because only eyes with exudative AMD were included in this study, the optimal degree of image compression in other disorders needs further investigation.
In summary, we investigated the influence of image compression in eyes with exudative AMD using Spectralis OCT. We revealed that 50% or better quality of the JPEG image may not influence the treatment decision. Although even a small amount of subretinal and intraretinal fluid can be detected in images with 25% of the quality of the JPEG, sufficient quality of choroidal images could be achieved in images with at least 50% of the quality of JPEG images. As a result, 50% of the quality of the JPEG images was found to have an optimal degree of compression in treating AMD when using the Spectralis OCT device. Investigating the influence of image compression in relation to other ophthalmologic devices and other retinal disorders would be of value.

References
Lee KH, Lee HJ, Kim JH, Kang HS, Lee KW, Hong H et al. Managing the CT data explosion: initial experiences of archiving volumetric datasets in a mini-PACS. J Digit Imaging 2005; 18: 188–195.
Rubin GD . Data explosion: the challenge of multidetector-row CT. Eur J Radiol 2000; 36: 74–80.
Woo HS, Kim KJ, Kim TJ, Hahn S, Kim B, Kim YH et al. JPEG 2000 compression of abdominal CT: difference in tolerance between thin- and thick-section images. AJR Am J Roentgenol 2007; 189: 535–541.
Flint AC . Determining optimal medical image compression: psychometric and image distortion analysis. BMC Med Imaging 2012; 12: 24.
Nassif N, Cense B, Park BH, Yun SH, Chen TC, Bouma BE et al. In vivo human retinal imaging by ultrahigh-speed spectral domain optical coherence tomography. Opt Lett 2004; 29: 480–482.
Manivannan A, Plskova J, Farrow A, McKay S, Sharp PF, Forrester JV . Ultra-wide-field fluorescein angiography of the ocular fundus. Am J Ophthalmol 2005; 140: 525–527.
Alam S, Zawadzki RJ, Choi S, Gerth C, Park SS, Morse L et al. Clinical application of rapid serial fourier-domain optical coherence tomography for macular imaging. Ophthalmology 2006; 113: 1425–1431.
Spaide RF, Koizumi H, Pozzoni MC . Enhanced depth imaging spectral-domain optical coherence tomography. Am J Ophthalmol 2008; 146: 496–500.
Baker CF, Rudnisky CJ, Tennant MT, Sanghera P, Hinz BJ, De Leon AR et al. JPEG compression of stereoscopic digital images for the diagnosis of diabetic retinopathy via teleophthalmology. Can J Ophthalmol 2004; 39: 746–754.
Basu A, Kamal AD, Illahi W, Khan M, Stavrou P, Ryder RE . Is digital image compression acceptable within diabetic retinopathy screening? Diabet Med 2003; 20: 766–771.
Conrath J, Erginay A, Giorgi R, Lecleire-Collet A, Vicaut E, Klein JC et al. Evaluation of the effect of JPEG and JPEG2000 image compression on the detection of diabetic retinopathy. Eye (Lond) 2007; 21: 487–493.
Rudnisky CJ, Tennant MT, Weis E, Ting A, Hinz BJ, Greve MD . Web-based grading of compressed stereoscopic digital photography versus standard slide film photography for the diagnosis of diabetic retinopathy. Ophthalmology 2007; 114: 1748–1754.
Tappeiner C, Barthelmes D, Abegg MH, Wolf S, Fleischhauer JC . Impact of optic media opacities and image compression on quantitative analysis of optical coherence tomography. Invest Ophthalmol Vis Sci 2008; 49: 1609–1614.
Sayanagi K, Sharma S, Yamamoto T, Kaiser PK . Comparison of spectral-domain versus time-domain optical coherence tomography in management of age-related macular degeneration with ranibizumab. Ophthalmology 2009; 116: 947–955.
Khurana RN, Dupas B, Bressler NM . Agreement of time-domain and spectral-domain optical coherence tomography with fluorescein leakage from choroidal neovascularization. Ophthalmology 2010; 117: 1376–1380.
Querques G, Forte R, Berboucha E, Martinelli D, Coscas G, Soubrane G et al. Spectral-domain versus time domain optical coherence tomography before and after ranibizumab for age-related macular degeneration. Ophthalmic Res 2011; 46: 152–159.
Kim JH, Kang SW, Ha HS, Kim SJ, Kim JR . Overestimation of subfoveal choroidal thickness by measurement based on horizontally compressed optical coherence tomography images. Graefes Arch Clin Exp Ophthalmol 2013; 251: 1091–1096.
Cukras C, Wang YD, Meyerle CB, Forooghian F, Chew EY, Wong WT . Optical coherence tomography-based decision making in exudative age-related macular degeneration: comparison of time- vs spectral-domain devices. Eye (Lond) 2010; 24: 775–783.
Chung SE, Kang SW, Lee JH, Kim YT . Choroidal thickness in polypoidal choroidal vasculopathy and exudative age-related macular degeneration. Ophthalmology 2011; 118: 840–845.
Koizumi H, Yamagishi T, Yamazaki T, Kawasaki R, Kinoshita S . Subfoveal choroidal thickness in typical age-related macular degeneration and polypoidal choroidal vasculopathy. Graefes Arch Clin Exp Ophthalmol 2011; 249: 1123–1128.
Ahn SJ, Woo SJ, Kim KE, Park KH . Association between choroidal morphology and anti-vascular endothelial growth factor treatment outcome in myopic choroidal neovascularization. Invest Ophthalmol Vis Sci 2013; 54 (3): 2115–2122.
Acknowledgements
This study is supported by Kim’s Eye Hospital Research Center.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Rights and permissions
About this article

Cite this article
Kim, J., Kang, S., Kim, Jr. et al. Influence of image compression on the interpretation of spectral-domain optical coherence tomography in exudative age-related macular degeneration. Eye 28, 825–831 (2014). https://doi.org/10.1038/eye.2014.102
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/eye.2014.102
