
Abstract
Tuberous sclerosis complex (TSC) is a rare autosomal dominant disorder characterized by hamartomas and hamartias in multiple organs. TSC is caused by a wide spectrum of mutations within the TSC1 and TSC2 genes. Here, we report a unique family with three independent pathological mutations in TSC2. A c.1322G>A mutation in exon 12 created a stop codon, whereas a second mutation in exon 23 (c.2713C>T) was a missense change. The third mutation was a 4 base pair deletion in intron 20 of TSC2. We showed that this mutation was responsible for abnormal splicing. The three mutations were most likely de novo, as parents of affected patients did not present any features of TSC. In addition, we showed gonadal mosaicism in a branch of the family. To our knowledge, several independent mutations in TSC2 have never been observed in a single family. The probability of finding a family with three different pathological TSC2 mutations is extremely low. We discuss two main hypotheses that may be raised to explain this recurrence: (i) the TSC2 mutation rate is underestimated. In such a case, the likelihood of finding a family with three independent mutations in TSC2 may not be dramatically low; (ii) a heritable defect in a DNA repair gene (eg, mismatch repair gene) segregating in the family that is unlinked to the TSC2 gene might predispose to the occurrence of multiple TSC2 gene mutations, used as a specific target during embryogenesis.
Similar content being viewed by others

Introduction
Tuberous sclerosis complex (TSC) is a rare autosomal dominant disorder, affecting ∼1 in 6000–10 000 individuals, caused by mutations within the TSC1 and TSC2 genes.1, 2 It is characterized by hamartomas and hamartias in multiple organs, such as brain, skin, heart, kidneys and lung.3 TSC often causes disabling neurological disorders, including epilepsy, mental retardation and autism. Additional major features of the disease include dermatological manifestations, cardiac rhabdomyomas, renal angiomyolipomas and pulmonary lymphangiomyomatosis. Although showing considerable variability in clinical expression, there is no evidence for non-penetrance when clinical and complementary investigations are carried out.4 However, three different missense mutations in TSC2 have been associated with unusually mild TSC features, including family members who carry the missense change and do not meet formal TSC diagnostic criteria.5, 6, 7
The TSC1 and TSC2 genes encode the protein products hamartin (130 kDa) and tuberin (200 kDa), respectively. The tumour-suppressor proteins, TSC1 and TSC2, function as a heterodimer for inhibiting cell growth and proliferation. In agreement with Knudson's two-hit tumour-suppressor gene model, inactivation of both the alleles of either TSC1 or TSC2 seems to be required for lesion formation in TSC.8
A wide spectrum of unique allelic variants in TSC2 has been reported. There are no particular regions in which mutations occur at a high rate, although the missense mutations tend to cluster in the GTPase-activating protein domain.9, 10, 11 The frequency of mutations reported in TSC2 is consistently higher than in TSC1. The germline mutation rate calculated for TSC (2.5 × 10−5) is one of the highest reported in humans.12 One consequence of this high mutation rate is that a majority of the TSC2 mutations occur de novo. Here, we report the molecular genetic analysis of a unique family with TSC, in which three independent disease-causing mutations in TSC2 have been identified.
Patients and methods
Patients and their relatives
Written informed consent was obtained from all participants. Clinical investigation included a review of medical history and a physical examination, with careful examination of the skin. Cerebral imaging (CT or MRI) was performed on individuals III-1, IV-2, IV-5, IV-16, V-1, V-3, V-10 and VI-3.
Haplotyping
For molecular studies, DNA was isolated from peripheral blood lymphocytes with standard methods. Linkage analysis was performed by the use of four (D9S179, D9S1830, D9S1793 and D9S164) and three (D16S521, D16S291 and D16S423) fluorescence-labelled polymorphic short tandem repeat (STR) markers located in the vicinity of TSC1 and TSC2, respectively.
DNA sequencing
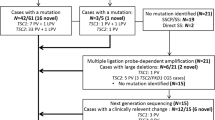
Polymerase chain reaction (PCR) amplifications, as well as sequencing of the coding regions and exon–intron boundaries of the TSC2 gene were performed on affected individuals IV-16, V-3 and VI-3. Exons 12, 20 and 23 and the corresponding exon–intron boundaries of the TSC2 gene were sequenced in individuals of the family (III-1, IV-2, IV-5, IV-9, IV-10, IV-11, IV-14, IV-15, IV-16, IV-18, IV-19, IV-20, V-1, V-2, V-4, V-5, V-8 and V-10). Exon 20 was sequenced on 100 unrelated and unaffected anonymous individuals.
RNA studies
Reverse transcription PCR (RT–PCR) was performed on RNA isolated from peripheral blood samples from patient VI-3 and an unrelated, unaffected anonymous individual was used as a control according to standard procedures. Subsequently, two independent PCRs were performed using the cDNA as a template (conditions available on request): (i) PCR with primers in exon 19 (E19F1-CTGTGCTCTGCTCTCTGCTCC) and in intron 20 (I20R-GCTAGAAGCACCAGGGAATCGG); and (ii) PCR with primers in exon 19 (E19F2-CATCTTTACTTCCCCTTGCAGTGTGG) and in exon 22 (E22R-GGCAAAGTTCCTGTAGAGGTGCGG). Electrophoresis was performed on polyacrylamide gel with RT–PCR products obtained from the patient and the control. E19-E22 PCR products were subcloned into the pGEM-T Easy vector (Promega) and re-amplified with the same pair of primers. The RT–PCR results were compared with the outcome of three different splice site prediction algorithms: Splice Site Finder; MaxEntScan (http://genes.mit.edu/burgelab/maxent/Xmaxentscan_scoreseq.html); and GeneSplicer (http://www.tigr.org/tdb/GeneSplicer/gene_spl.html) We simultaneously investigated Splice Site Finder, MaxEntScan and GeneSplicer using the software Alamut (Interactive Biosoftware; http://www.interactive-biosoftware.com).
Results
Five (IV-16, V-3, V-8, V-10 and VI-3) of the 92 individuals of this French family presented with features leading to the diagnosis of TSC (Table 1). One additional deceased individual (IV-12) was affected according to his medical history. Clinical and complementary examinations excluded the diagnosis of TSC in four individuals (III-1, IV-2, IV-5 and V-1). Linkage analysis excluded the TSC1 locus (data not shown). Using three STR markers in the vicinity of TSC2, a common haplotype was observed for three affected individuals (IV-16, V-8 and V-10) belonging to the same branch of the family, but not for the other two affected patients (V-3 and VI-3) (Figure 1). These results were against the hypothesis of a single TSC1 or TSC2 mutation segregating in the family.

Simplified pedigree of the family (the entire pedigree contains 92 individuals) showing three-locus genotypes and inferred haplotypes. Genotypes are shown in the following order, from top to bottom: D16S521, D16S291 and D16S423. The same haplotype (shown in the black square) carried by three affected individuals (IV-16, V-8 and V-10) was also identified in two healthy sisters (IV-9 and IV-15) of patient IV-16 consistent with gonadal mosaicism. The arrow indicates the location of TSC2 between D16S521 and D16S291. Clear symbols denote unaffected individuals and black symbols denote clinically affected individuals. c.1322 G>A, mutation identified in patients IV-16, V-8 and V-10; c.2713 C>T, mutation identified in patient V-3; IVS20+1-4 delGTAG, mutation identified in patient VI-3. The symbol ‘−’ indicates the absence of mutation identified in TSC2.
The mutation analysis of TSC2 identified a novel c.1322G>A (p.Trp441X) stop mutation in exon 12 in the three patients (IV-16, V-8 and V-10) belonging to the same branch of the family, in which linkage analysis showed a common haplotype. A different mutation, c.2713C>T (p.Arg905Trp), in exon 23 of TSC2 was identified in patient V-3. This missense mutation was observed in earlier published reports on patients with TSC.5, 9, 13, 14, 15, 16, 17 Finally, a third independent mutation (IVS20+1-4 delGTAG) in TSC2 was identified in patient VI-3. This 4 base pair (bp) deletion removes the natural splice donor site of intron 20 at the junction between exon 20 and intron 20. The mutation was not found in 200 chromosomes from the 100 unrelated and unaffected individuals. To confirm the pathological effect of the mutation, RT–PCR was performed on RNA isolated from peripheral blood samples from patient VI-3. cDNA was used as a template for PCR using primers in exon 19 and intron 20. An aberrant 342-bp amplified fragment consisted of exons 19 and 20 followed by intron 20 in the patient, whereas no amplified product was obtained from the cDNA control (Figure 2a–c). The product led to a stop codon in position 821 of intron 20. In addition, PCR was performed using primers in exons 19 and 22. Polyacrylamide gel electrophoresis, using the cDNA control, showed a single band corresponding to the expected normal 418-bp sequence. Using the cDNA of the patient, two close bands with similar intensities were observed. One band corresponded to the normal 418-bp amplified product, whereas the second band most likely corresponded to abnormal splicing products (Figure 2a). Subsequently, subcloning and re-amplification with the same pair of primers and sequencing characterized two additional aberrant cDNA products. Two novel cryptic splice donor sites in intron 20 were utilized, leading to a 421- and 476-bp amplified products. The 421-bp amplified product was identified in 2 clones among 12 sequenced clones, and consisted of exons 19 and 20, 3 bp of intron 20 and exons 21 and 22 (Figure 2d and e). The 476-bp amplified product was identified in 4 clones and consisted of exons 19 and 20, 58 bp of intron 20 and exons 21 and 22 (data not shown). The remaining six sequenced clones were normal. Three different algorithms (Splice Site Finder, MaxEntScan and GeneSplicer) were used to test whether the results obtained by using the RT–PCR analysis of patient RNA could have been predicted in silico. All algorithms predicted that the mutation would lead to an elimination of the intron 20 donor site and to the generation of two strong novel cryptic splice donor sites in intron 20, those that we observed experimentally (see Supplementary Table S1 online).

(a) Left panel: RT–PCR analysis using primers in exon 19 and in intron 20. An aberrant 342-bp amplified fragment consisted of exons 19 and 20 followed by intron 20 in patient VI-3 carrying the IVS20+1–4 delGTAG mutation, whereas no amplified product was obtained from the cDNA control. Right panel: RT–PCR analysis using primers in exon 19 and exon 22. Using the cDNA control, a single band corresponding to the expected normal 418-bp sequence was observed. Using the cDNA of patient VI-3, two close bands with similar intensities were observed. One band corresponded to the normal 418-bp amplified product, whereas the second band corresponded to abnormal splicing products. L, small fragment ladder; VI-3, RT–PCR using cDNA of the affected patient VI-3; C, RT–PCR using cDNA of an anonymous unaffected individual used as a control. (b) Wild-type genomic sequence of the TSC2 exon 20–intron 20 junction. Four base pairs (GTAG), deleted in the mutated allele, are shown in bold. (c) Sequence chromatograms from cDNA of patient VI-3 using primers in exon 19 and in intron 20. An aberrant product consisted of exons 19 and 20 followed by intron 20 with a 4 base pair (GTAG) deletion leading to a stop codon in intron 20. (d) Wild-type genomic sequence of the TSC2 exon 20–intron 20 and intron 20–exon 21 junctions. Four base pairs (GTAG), deleted in the mutated allele, are shown in bold. A novel GT cryptic splice donor site in intron 20 is shown in the square. (e) Sequence chromatograms from cDNA of patient VI-3 using primers in exons 19 and 22 after subcloning. An abnormal product consisted of exons 19 and 20, 3 base pairs of intron 20 and exons 21 and 22. gDNA, genomic DNA; cDNA, complementary DNA; E, exon; I, intron; del 4 bp, 4 base pair deletion.
Sequencing excluded the three different mutations in healthy individuals of the family (III-1, IV-2, IV-5, IV-9, IV-10, IV-11, IV-14, IV-15, IV-16, IV-18, IV-19, IV-20, V-1, V-2, V-4 and V-5). Among these individuals, the parents of patient VI-3 did not carry the splice site mutation proving a de novo event in this patient. The p.Arg905Trp missense mutation that was identified in patient V-3 was most likely de novo, as both parents had no features of TSC and the mutation was absent from the patient's mother. However, as no DNA was available from the patient's father, the mutation still might be paternally inherited. Finally, a stop mutation (p.Trp441X) was identified in patient IV-16. One deceased brother presented with TSC, whereas none of the other eight brothers and sisters of patient IV-16 presented with features suggestive of TSC. Sequencing excluded the stop mutation in these eight brothers and sisters, whereas it was identified in two additional affected patients belonging to the same branch of the family (V-8 and V-10). The same haplotype carried by the three affected individuals (IV-16, V-8 and V-10) was also identified in two healthy sisters with no mutation (IV-9 and IV-15) of patient IV-16, suggesting that there had been gonadal mosaicism in one of the parents (III-3 or III-4).
Discussion
We report a unique family with three independent pathological mutations in TSC2 mapping to distinct haplotypes. One mutation created a stop codon, whereas a second mutation was a missense change. The third mutation was a 4-bp deletion at the splice site of intron 20 of TSC2. The three mutations were most likely de novo, as parents of the affected patients did not present any features of TSC. In addition, findings consistent with gonadal mosaicism were seen in one branch of the family, which is known to occur in TSC.18 The three mutations were most likely to have been generated by different mutational mechanisms. The 4-bp deletion may have occurred by slipped strand mispairing. The missense mutation, a C to T transition in exon 23 reported 19 times earlier (http://chromium.liacs.nl/LOVD2/TSC/home.php?select_db=TSC2), occurred at a hypermutable CpG motif, most likely mediated by methylation-mediated deamination. The nonsense mutation, a G>A transition, has not been reported earlier.
Two independent mutations, one in TSC1 and the other in TSC2, have been reported earlier in a family with TSC.4, 19 However, to our knowledge, several independent mutations in TSC2 have never been observed in a single family. The probability of finding a family with three different pathological TSC2 mutations is extremely low. The estimation of the probability of finding a family with three independent, non-identical, pathological TSC2 mutations occurring de novo in 92 relatives and considering a mutation rate of 2.5 × 10−5 is ∼2.6 × 10−6 or, in other words, 1 in ∼500 000 000 families of 92 individuals (see Supplementary Note online).
Two main hypotheses may be raised to explain this TSC2 gene mutation recurrence. Interestingly, the same reasoning was used to explain a neurofibromatosis type 1 (NF1) family with three different pathological mutations originating de novo in the NF1 gene.20 NF1 is a complex autosomal disorder, affecting ∼1 in 3500 individuals, linked to the NF1 gene mutations of which 50% are de novo mutations.21
-
i)
The likelihood of finding a family with three independent mutations in the TSC2 gene may not be dramatically low, because the mutation rate in this gene is underestimated. If the penetrance of the TSC2 gene mutations was incomplete, heterozygous mutations might occur in clinically asymptomatic individuals; then, the actual prevalence of the TSC2 gene mutations in the general population might be considerably higher than the current estimates. However, subclinical or unrecognized TSC is extremely rare, when an experienced clinician evaluates the patient with modern diagnostic imaging. Three missense mutations in TSC have been associated with a milder clinical phenotype, but in aggregate these account for <1% of all the TSC mutations.
-
ii)
There may be a heritable defect in DNA repair segregating in the family that is unlinked to the TSC2 gene, but which is responsible for the occurrence of multiple TSC2 gene mutations. A number of tumour-suppressor genes, whose normal function is to maintain genome stability and integrity, have been identified. Mutation in these genes can compromise basic cellular processes, such as replication fidelity, DNA repair, cell arrest or apoptosis, thereby promoting genomic instability. In our family, we did not observe any unusual recurrence of cancer or neurodegenerative disorders in the affected TSC patients or in the unaffected individuals. In addition, no microsatellite instability was observed when using the STR markers for linkage analysis. On the basis of this hypothesis, TSC2 would be a highly specific mutational target for a DNA repair gene. In addition, the mutations that have occurred in this family are of different types.
Over the past few years, bi-allelic mismatch repair (MMR) gene mutations have been identified in 15 families with the association of neurofibromatosis features and early onset of childhood malignancies.22, 23 Homozygous or compound heterozygous mutations affecting the MLH1, MSH2, MSH6 or PMS2 genes have been reported in such patients. Neurofibromatosis features have not been detected in the parents of these patients, strongly suggesting that this particular form of neurofibromatosis is caused by MMR deficiency leading to a NF1 mutation. Several studies provided convincing data supporting the hypothesis that MMR deficiency and neurofibromatosis may be associated with NF1 mutations. The NF1 gene is often mutated in DNA MMR-deficient cancer cell lines, as well as in primary tumours exhibiting microsatellite instability.24 Moreover, the NF1 gene alterations in Mlh1(−/−) mouse embryonic fibroblasts provided additional evidence that the Nf1 gene may be a mutational target in MMR-deficient cells. Finally, recently a child presenting with NF1 and early onset leukaemia showed a heterozygous NF1 gene mutation in addition to a homozygous MLH1 gene mutation.23 The parents did not show NF1 features or the NF1 mutation. Therefore, the occurrence of the de novo NF1 mutation that was identified in the child may have been facilitated by DNA MMR deficiency because of the inherited homozygous MLH1 mutation in the affected child.
Although there are some parallels between these reports and the family reported here, there are several discordances. First, there were no other tumours or neurodegenerative syndromes seen in this family. Second, standard vertical transmission of TSC2 mutations was seen in at least one branch of this family.
Therefore, we suspect that this family represents a rare, highly statistically unlikely aggregation of novel mutations in the TSC2 gene in three generations. Nonetheless, there is a possibility that a mutation in a DNA repair or other gene segregating in this family might have predisposed to recurrent TSC2 mutations.
References
European Chromosome 16 Tuberous Sclerosis Consortium: Identification and characterization of the tuberous sclerosis gene on chromosome 16. Cell 1993; 75: 1305–1315.
van Slegtenhorst M, de Hoogt R, Hermans C et al: Identification of the tuberous sclerosis gene TSC1 on chromosome 9q34. Science 1997; 277: 805–808.
Crino PB, Nathanson KL, Henske EP : The tuberous sclerosis complex. N Engl J Med 2006; 355: 1345–1356.
Osborne JP, Jones AC, Burley MW et al: Non-penetrance in tuberous sclerosis. Lancet 2000; 355: 1698.
Jansen AC, Sancak O, D’Agostino MD et al: Unusually mild tuberous sclerosis phenotype is associated with TSC2 R905Q mutation. Ann Neurol 2006; 60: 528–539.
Khare L, Strizheva GD, Bailey JN et al: A novel missense mutation in the GTPase activating protein homology region of TSC2 in two large families with tuberous sclerosis complex. J Med Genet 2001; 38: 347–349.
O’Connor SE, Kwiatkowski DJ, Roberts PS, Wollmann RL, Huttenlocher PR : A family with seizures and minor features of tuberous sclerosis and a novel TSC2 mutation. Neurology 2003; 61: 409–412.
Knudson Jr AG : Mutation and cancer: statistical study of retinoblastoma. Proc Natl Acad Sci USA 1971; 68: 820–823.
Jones AC, Shyamsundar MM, Thomas MW et al: Comprehensive mutation analysis of TSC1 and TSC2-and phenotypic correlations in 150 families with tuberous sclerosis. Am J Hum Genet 1999; 64: 1305–1315.
Dabora SL, Jozwiak S, Franz DN et al: Mutational analysis in a cohort of 224 tuberous sclerosis patients indicates increased severity of TSC2, compared with TSC1, disease in multiple organs. Am J Hum Genet 2001; 68: 64–80.
Maheshwar MM, Cheadle JP, Jones AC et al: The GAP-related domain of tuberin, the product of the TSC2 gene, is a target for missense mutations in tuberous sclerosis. Hum Mol Genet 1997; 6: 1991–1996.
Sampson JR, Scahill SJ, Stephenson JB, Mann L, Connor JM : Genetic aspects of tuberous sclerosis in the west of Scotland. J Med Genet 1989; 26: 28–31.
Yamashita Y, Ono J, Okada S et al: Analysis of all exons of TSC1 and TSC2 genes for germline mutations in Japanese patients with tuberous sclerosis: report of 10 mutations. Am J Med Genet 2000; 90: 123–126.
Sancak O, Nellist M, Goedbloed M et al: Mutational analysis of the TSC1 and TSC2 genes in a diagnostic setting: genotype–phenotype correlations and comparison of diagnostic DNA techniques in tuberous sclerosis complex. Eur J Hum Genet 2005; 13: 731–741.
Au KS, Rodriguez JA, Finch JL et al: Germ-line mutational analysis of the TSC2 gene in 90 tuberous-sclerosis patients. Am J Hum Genet 1998; 62: 286–294.
Au KS, Williams AT, Roach ES et al: Genotype/phenotype correlation in 325 individuals referred for a diagnosis of tuberous sclerosis complex in the United States. Genet Med 2007; 9: 88–100.
Yamamoto T, Pipo JR, Feng JH et al: Novel TSC1 and TSC2 mutations in Japanese patients with tuberous sclerosis complex. Brain Dev 2002; 24: 227–230.
Rose VM, Au KS, Pollom G, Roach ES, Prashner HR, Northrup H : Germ-line mosaicism in tuberous sclerosis: how common? Am J Hum Genet 1999; 64: 986–992.
Webb DW, Osborne JP : Non-penetrance in tuberous sclerosis. J Med Genet 1991; 28: 417–419.
Upadhyaya M, Majounie E, Thompson P et al: Three different pathological lesions in the NF1 gene originating de novo in a family with neurofibromatosis type 1. Hum Genet 2003; 112: 12–17.
Huson SM, Compston DA, Clark P, Harper PS : A genetic study of von Recklinghausen neurofibromatosis in south east Wales. I. Prevalence, fitness, mutation rate, and effect of parental transmission on severity. J Med Genet 1989; 26: 704–711.
Bandipalliam P : Syndrome of early onset colon cancers, hematologic malignancies and features of neurofibromatosis in HNPCC families with homozygous mismatch repair gene mutations. Fam Cancer 2005; 4: 323–333.
Alotaibi H, Ricciardone MD, Ozturk M : Homozygosity at variant MLH1 can lead to secondary mutation in NF1, neurofibromatosis type I and early onset leukemia. Mutat Res 2008; 637: 209–214.
Wang Q, Montmain G, Ruano E et al: Neurofibromatosis type 1 gene as a mutational target in a mismatch repair-deficient cell type. Hum Genet 2003; 112: 117–123.
Acknowledgements
We are grateful to the patients for their participation in this study.
Author information
Authors and Affiliations
Corresponding author
Additional information
Conflict of interest
The authors declare no conflict of interest.
Supplementary Information accompanies the paper on European Journal of Human Genetics website (http://www.nature.com/ejhg)
Supplementary information
Rights and permissions
About this article
Cite this article
Le Caignec, C., Kwiatkowski, D., Küry, S. et al. Three independent mutations in the TSC2 gene in a family with tuberous sclerosis. Eur J Hum Genet 17, 1165–1170 (2009). https://doi.org/10.1038/ejhg.2009.28
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/ejhg.2009.28
