
The idea behind digital contact tracing is that, when an individual tests positive for an infectious disease such as COVID-19, an app on their smartphone can send a notification to other smartphones that have been in close proximity, such as within 2 metres, for more than a certain period of time, say 15 minutes. However, such apps can be difficult for people living in a democracy to accept because of concerns about data privacy. Writing in Nature, Wymant et al.1 demonstrate effective implementation of a digital contact-tracing app on a large scale in a democratic society: England and Wales in the United Kingdom.
Read the paper: The epidemiological impact of the NHS COVID-19 App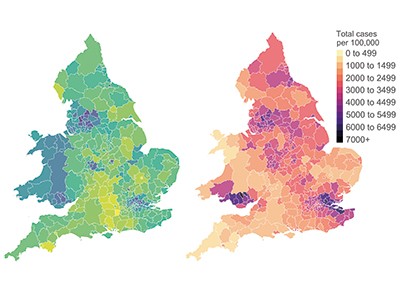
The technology used in the app, which was named the NHS COVID-19 app after Britain’s National Health Service, is the Google Apple Exposure Notification (GAEN) system. This uses low-energy Bluetooth-enabled radio signals to send a randomly generated identification code from one phone to another that is in close proximity, creating a sort of ‘handshake’; these codes change every 10–20 minutes. The codes of phones that have been in close physical contact over the previous 14 days are stored in the app on a user’s phone. When a user tests positive for COVID-19, they can consent to have their codes sent anonymously to a central server. Other app users can sync with the central server for a match. Thus, the app can help to alert people who have potentially been exposed to COVID-19, so that they can then get tested, voluntarily place themselves in quarantine and inform their contacts that they should do the same.
A contact-tracing app will make a meaningful difference in the population only if a large enough proportion install and use it. The NHS COVID-19 app experience shows that there is enough participation in app use for it to be useful. An estimated 33.9 million people were eligible to download the app (that is, they were aged 16 or over, were located in England or Wales and had a compatible smartphone). Between its launch on 24 September 2020 and the end of 2020, the app was downloaded on 21 million separate devices and, between 1 November and 11 December 2020, it was regularly used by an average of about 16.5 million users, which is about 49% of the eligible population, or 28% of the total population of England and Wales. Moreover, 72% of app-using ‘index’ cases (individuals who tested positive for COVID-19) consented to an app-based exposure notification being sent after testing positive.
Knowing that a randomized, controlled trial of a digital contact-tracing app is probably not feasible, Wymant et al. used two ways of estimating the impact of the app on the spread of COVID-19 from October to December 2020. First, using the number of observed notifications and the secondary attack rate — the proportion of contacts identified who ended up becoming infected — they modelled the number of cases averted as a result of app use. Second, they performed statistical comparisons of cumulative cases in neighbouring regions that had similar baseline infection rates but differing levels of app use, after adjusting for factors known to correlate with app uptake (such as areas being more rural, and having less poverty and a stronger local economy) and with infection rate.
The authors estimated that, for every 1% increase in app users, the number of cases could be reduced by 0.8% (from modelling), or by 2.3% (from statistical comparisons; Fig. 1). The authors also estimated the probability that someone who received a notification would test positive in the following 2 weeks to be 6%. Overall, approximately one new case was averted for each individual with confirmed COVID-19 who consented to their contacts being notified through the app.

Figure 1 | Estimated effects of a contact-tracing app on cases of COVID-19. Wymant et al.1 used two approaches to examine the possible effect on the spread of COVID-19 of a contact-tracing app deployed in England and Wales. a, First, they used modelling to estimate that the percentage of cases of COVID-19 averted in each local region (each region represented by a data point) increased by 0.8% for every percentage-point increase in app uptake. b, Second, the authors compared the numbers of COVID-19 cases per 1,000 people in similar, neighbouring regions that showed differences in app uptake. The comparison suggested that, for every 1% increase in app uptake, there was a 2.3% reduction in cases. The red-shaded areas represent 95% confidence intervals.
The estimated effect of the app on reducing spread of the disease is particularly remarkable given that COVID-19 testing was not mandatory, and self-isolation or quarantine was not strictly enforced for index cases or for those who were notified. In a series of UK surveys, among those who reported symptoms of COVID-19 in a 7-day period, only 20.2% reported having isolated fully, although around 70% intended to adhere to the rules if symptoms developed2.
A common criticism of digital contact tracing is that it could create a lot of ‘noise’, by contacting a large number of individuals who have a low chance of having been infected, compared with the contacts identified by human (or ‘manual’) contact tracers, whose detailed interviews might be more likely to reach true close contacts. Wymant et al. showed that the secondary attack rate of 6% for the app is similar to the 6.9% rate achieved by manual contact tracing (see go.nature.com/2qxkkzf). They also found that the mean number of contacts reached was 4.4 for digital tracing, compared with 1.8 for manual tracing, with the app thought to have reached more contacts outside an individual’s household than did manual tracing. This strongly supports the idea that the app is as accurate as, and can be complementary to, manual contact tracing.
Big data and simple models used to track the spread of COVID-19 in cities
As mentioned above, digital contact tracing raises privacy concerns. Many citizens simply do not wish to be tracked for their health status, particularly when their freedom to travel might be compromised as a result3. However, the technology used in GAEN anonymizes the data and keeps them private in users’ phones. Furthermore, an infected person must consent for the codes to be sent to the central server to allow contact matching. The identification codes cannot be used by someone at the central server to reveal the identity of the infected person or their contacts.
The main advantages of digital contact tracing are the speed and scalability it offers. This is particularly relevant to COVID-19, because individuals can transmit the SARS-CoV-2 virus for several days before developing symptoms, or can simply remain asymptomatic4. Contact-tracing apps might work more quickly and more reliably than manual approaches that involve interviewing infected people, many of whom do not keep track of their recent contacts and forget them. Another advantage of digital contact tracing is its ability to contact strangers; it is otherwise simply not possible to track down strangers who sat near an infected person on a bus.
The NHS COVID-19 app now has extra features. These include: the ability to ‘check in’ at a venue by scanning its QR code (a type of barcode) for later notification if the venue has positive cases; a symptom tracker that is linked to a test-booking system; and the ability to order tests and receive results through the app.
An estimation of undetected COVID cases in France
To be maximally effective, digital contact tracing relies on the health system’s ability to follow up on potential contacts and offer them testing, clinical care and social and material support during quarantine, as needed. The flow of data can also strongly affect the efficacy of digital contact tracing. For example, are positive test results self-reported to the app or directly obtained or auto-populated from the test laboratories? Will health-care providers and public-health officials be quickly informed about positive test results so that they can act quickly in contact tracing, advising quarantine and testing for close contacts, and providing support and care for infected individuals? All these elements can contribute to the effectiveness of both digital and manual contact-tracing efforts.
Although health officials in England and Wales are not made aware of the identities of infected individuals from the app, they can use data from the app to estimate infection rates in the postcode district (the first half of the postcode) that is entered by users during the app registration process. Given these restrictions and the focus on privacy and autonomy (that is, with users having the choice of whether or not to send a positive-test notification), it is remarkable that the contact-tracing app still showed impressive results in mitigating the spread of COVID-19. The success of the NHS COVID-19 app offers hope that other digital contact-tracing apps might prove to be useful elsewhere, offering new capabilities in containing the spread of a rapidly spreading virus.
 Read the paper: The epidemiological impact of the NHS COVID-19 App
Read the paper: The epidemiological impact of the NHS COVID-19 App
 Big data and simple models used to track the spread of COVID-19 in cities
Big data and simple models used to track the spread of COVID-19 in cities
 An estimation of undetected COVID cases in France
An estimation of undetected COVID cases in France



