
Abstract
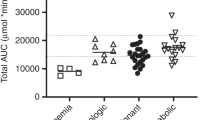
In solid organ transplantation, CYA dosing is based on the area under the concentration vs time curve (AUCinf). This study aimed to develop a guideline for the initial i.v. CYA dose for pediatric hematopoietic SCT (HSCT) patients to achieve the target AUCinf recommended in solid organ transplantation. Whole-blood CYA concentrations were determined in 24 patients (0.5–16.9 years) after the first i.v. dose given over 2 h, 1 day before HSCT. The i.v. CYA dose predicted to achieve an AUCinf of 4200 μg × h/l was calculated for each patient and expressed as a function of each patient's actual weight and body surface area (BSA). In patients ⩽9 and >9 years of age, the mean i.v. CYA dose predicted to achieve the target AUC was 2.6±0.94 and 2.1±1.21 mg/kg, respectively. When these doses were expressed in terms of BSA, the mean dose was 65±23.1 and 68±35.0 mg/m2 in children ⩽9 and >9 years of age, respectively. In children 0.5–17 years of age undergoing HSCT, we recommend an initial i.v. CYA dose of 65 mg/m2 infused over 2 h to achieve an AUCinf of approximately 4200 μg × h/l.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others

References
Ruutu T, Niederwieser D, Gratwohl A, Apperley JF . A survey of the prophylaxis and treatment of acute GVHD in Europe: a report of the European Group for Blood and Marrow, Transplantation (EBMT). Chronic Leukaemia Working Party of the EBMT. Bone Marrow Transplant 1997; 19: 759–764.
Hoppu K, Koskimies O, Holmberg C, Hirvisalo EL . Pharmacokinetically determined cyclosporine dosage in young children. Pediatr Nephrol 1991; 5: 1–4.
Ptachinski RJ, Burckart GJ, Rosenthal JT, Venkataramanan R, Howrie DL, Taylor RJ et al. Cyclosporine pharmacokinetics in children following cadaveric renal transplantation. Transplant Proc 1986; 18: 766–767.
Mahalati K, Belitsky P, Sketris I, West K, Panek R . Neoral monitoring by simplified sparse sampling area under the concentration–time curve: its relationship to acute rejection and cyclosporine nephrotoxicity early after kidney transplantation. Transplantation 1999; 68: 55–62.
Lindholm A, Kahan BD . Influence of cyclosporine pharmacokinetics, trough concentrations, and AUC monitoring on outcome after kidney transplantation. Clin Pharmacol Ther 1993; 54: 205–218.
Filler G, Mai I, Filler S, Ehrich JH . Abbreviated cyclosporine AUCs on Neoral—the search continues!. Pediatr Nephrol 1999; 13: 98–102.
Duncan N, Craddock C . Optimizing the use of cyclosporin in allogeneic stem cell transplantation. Bone Marrow Transplant 2006; 38: 169–174.
Nawa Y, Hara M, Tanimoto K, Nakase K, Kozuka T, Maeda Y . Single-dose daily infusion of cyclosporine for prevention of graft-versus-host-disease after allogeneic bone marrow transplantation from HLA allele-matched, unrelated donors. Int J Hematol 2006; 83: 159–163.
Hendriks MP, Blijlevens NM, Schattenberg AV, Burger DM, Donnelly JP . Cyclosporine short infusion and C2 monitoring in haematopoietic stem cell transplant recipients. Bone Marrow Transplant 2006; 38: 521–525.
Barkholt L, Remberger M, Bodegard H, Ringden O, Bottiger Y . Cyclosporine A (CSA) 2-h concentrations vary between patients without correlation to graft-versus-host disease after allogeneic haematopoietic stem cell transplantation. Bone Marrow Transplant 2007; 40: 683–689.
Izumi N, Furukawa T, Sato N, Okazuka K, Tsukada N, Abe T et al. Risk factors for acute graft-versus-host disease after allogeneic hematopoietic stem cell transplantation: retrospective analysis of 73 patients who received cyclosporine A. Bone Marrow Transplant 2007; 40: 875–880.
Dupuis LL, Taylor T, Saunders EF . Disposition of two oral formulations of cyclosporine in pediatric patients receiving hematopoietic stem cell transplants. Pharmacotherapy 2006; 26: 15–22.
Giesbrecht E, Soldin S, Wong P . A reliable high-performance liquid chromatographic micromethod for the measurement of cyclosporine in whole blood. Ther Drug Monit 1989; 11: 332–336.
Belitsky P, Mahalati K, West K, Sketris I . Influence of drug formulation on utilization and outcomes: Neoral and monitoring by sparse sample area under the curve. Transplant Proc 1999; 31: 1667–1668.
Trompeter R, Fitzpatrick M, Hutchinson C, Johnston A . Longitudinal evaluation of the pharmacokinetics of cyclosporin microemulsion (Neoral™) in pediatric renal transplant recipients and assessment of C2 level as a marker for absorption. Pediatr Transplant 2003; 7: 282–288.
Keown PA, Kahan BD, Johnston A, Levy G, Dunn SP, Cittero F et al. Optimization of cyclosporine therapy with new therapeutic drug monitoring strategies: report from the International Neoral TDM Advisory Consensus Meeting. Transplant Proc 1998; 30: 1645–1649.
Peters C, Minkov M, Gadner H, Klingebiel T, Vossen J, Locatelli F et al. Statement of current majority practices in graft-versus-host disease prophylaxis and treatment in children. Bone Marrow Transplant 2000; 26: 405–411.
Schwinghammer TL, Bloom EJ, Rosenfeld CS, Wilson JW, Przepiorka D, Shadduck RK . High-dose cyclosporine and corticosteroids for prophylaxis of acute and chronic graft-versus-host disease. Bone Marrow Transplant 1995; 16: 147–154.
Murry DJ, Crom WR, Reddick WE, Bhargava R, Evans WE . Liver volume as a determinant of drug clearance in children and adolescents. Drug Metab Dispos 1995; 23: 1110–1116.
Willemze A, Cremers S, Schoemaker R, Lankester A, den Hartigh J, Burggraaf K et al. Cyclosporine A kinetics in children after stem cell transplantation [abstract]. Blood 2006; 108: 826a.
Acknowledgements
Sources of financial support: This study was partially supported by an unrestricted grant from Novartis Pharmaceuticals Canada Inc., Dorval, Quebec, Canada.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Jin, M., Seto, W., Taylor, T. et al. Determination of initial i.v. CYA dosage to achieve target AUC values in pediatric hematopoietic stem cell transplant patients. Bone Marrow Transplant 42, 455–459 (2008). https://doi.org/10.1038/bmt.2008.189
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bmt.2008.189
