
Abstract
Relapse and acquired drug resistance in T-cell acute lymphoblastic leukemia (T-ALL) remains a significant clinical problem. This study was designed to establish a preclinical model of resistance to induction therapy in childhood T-ALL to examine the emergence of drug resistance and identify novel therapies. Patient-derived T-ALL xenografts in immune-deficient (non-obese diabetic/severe combined immunodeficient) mice were exposed to a four-drug combination of vincristine, dexamethasone (DEX), L-asparaginase and daunorubicin (VXLD). ‘Relapse’ xenografts were characterized by responses to drugs, changes in gene expression profiles and Connectivity Map (CMap) prediction of strategies to reverse drug resistance. Two of four xenografts developed ex vivo and in vivo drug resistance. Both resistant lines showed altered lipid and cholesterol metabolism, yet they had a distinct drug resistance pattern. CMap analyses reinforced these features, identifying the cholesterol pathway inhibitor simvastatin (SVT) as a potential therapy to overcome resistance. Combined ex vivo with DEX, SVT was significantly synergistic, yet when administered in vivo with VXLD it did not delay leukemia progression. Synergy of SVT with established chemotherapy may depend on higher drug doses than are tolerable in this model. Taken together, we have developed a clinically relevant in vivo model of T-ALL suitable to examine the emergence of drug resistance and to identify novel therapies.
Similar content being viewed by others


Introduction
Acute lymphoblastic leukemia (ALL) is the most common childhood malignancy, constituting approximately 80% of pediatric leukemia and nearly 30% of all childhood cancers.1,2 Recent advances in the treatment of pediatric ALL have resulted in increased cure rates to around 85% in the developed world.3 Better outcome for patients is the result of more intensive combination chemotherapies and improvements in supportive care. These protocols include the administration of multiple chemotherapeutic drugs over a period of at least 2 years.4 Treatment is comprised of an initial remission-induction therapy (4–5 weeks) followed by intensification or consolidation therapy (~12–26 weeks), re-induction and then maintenance therapy (up to 3 years) to achieve cure.5 Up to 11 different chemotherapeutic drugs are used, yet it is the response to the agents administered during remission induction therapy that is a major prognostic factor in childhood ALL.6, 7, 8 Typically, they comprise vincristine (VCR), L-asparaginase (ASP), the glucocorticoids dexamethasone (DEX) or prednisone, with or without an anthracycline such as daunorubicin (DNR). Despite the induction treatment resulting in complete remission rates of >95%,3 up to 20% of pediatric ALL patients relapse and these individuals experience only a 30–50% likelihood of survival.9 Specifically, although T-cell ALL (T-ALL) represents only 10–15% of all pediatric ALL, it constitutes up to 48% of high-risk patients.9,10 Moreover, patients who relapse early in the bone marrow (BM; within 18–24 months), as is the case for the majority of T-ALL relapses, experience a dismal outcome.9,11 Relapsed ALL is thus a leading cause of cancer-related deaths in children.
Resistance to remission induction drugs, particularly the glucocorticoids, confers poor prognosis in relapsed ALL.12,13 Understanding the mechanisms underlying development of drug resistance is critical to develop more effective treatment regimens. Pre-clinical models are essential to explore cancer biology, drug resistance mechanisms and to evaluate new drugs. Cell line-derived in vitro models are well established for pre-clinical drug development, however, their ability to recapitulate primary disease is limited. In contrast, in vivo xenograft models closely resemble their tumor type of origin and more accurately predict the clinical activity of novel compounds in patients, thus the increased use of patient-derived xenografts for pre-clinical modeling.14 For studying ALL, the non-obese diabetic/severe combined immunodeficient (NOD/SCID) model is well established and allows direct transplantation of leukemia cells from patients.15,16 Importantly, the phenotype, genotype and kinetics of engraftment into the NOD/SCID mice appear to reflect the human disease with BM infiltration, followed by migration to the spleen, peripheral blood and other hematopoietic organs.16,17 Moreover, the model demonstrates the clinical relevance of gene expression profiling in ALL.18 Continuous xenografts can be established by transplanting cells harvested from the spleens of engrafted mice into secondary and tertiary recipient mice, which allows the measurement in vivo of the effect of drugs or drug combinations, and drug resistance mechanisms.19,20
The aim of the current study was to develop a pre-clinical model of induction therapy for pediatric ALL in NOD/SCID mice so that it can be used to study the development of drug resistance in vivo and identify alternative therapeutic approaches. We established four T-ALL xenografts from patient samples and mice were treated with an induction-type regimen consisting of VCR, DEX, ASP and DNR (VXLD) in one or more blocks. The resulting outgrowths of two ‘relapsed’ xenografts were subjected to comprehensive drug testing and gene expression profiling. Using Connectivity Map (CMap) analysis,20,21 we identified simvastatin (SVT) as a potential resistance-reversing drug, known to inhibit cholesterol synthesis via the mevalonic acid pathway.22 In this study, we provide proof of concept that the model is suitable to identify alternative therapeutic approaches, and our findings highlight the importance of in vivo validation.
Materials and methods
Development of T-ALL xenografts and in vivo drug treatments
All experimental studies had received prior approval from the Animal Care and Ethics Committee of the University of New South Wales, and the Human Research Ethics Committees of the South Eastern Sydney Local Health District and the University of New South Wales. Samples used in this study were obtained from children treated in Australia and New Zealand Children’s Haematology and Oncology Group (ANZCHOG) Study 8 clinical trial (http://www.anzctr.org.au/trial_view.aspx?ID=1568), with the exception of sample ALL-29 obtained from a Study 7 patient. Xenograft lines were established from T-ALL diagnosis biopsy samples in the NOD/SCID strain as previously described,16 and patient demographics are detailed in Table 1. Methods for monitoring engraftment and disease progression, in vivo selection of xenograft lines with VXLD and in vivo drug efficacy are detailed in the Supplementary Materials and Methods.
MTT colorimetric assay
Xenograft cells were assessed for single agent and combination ex vivo drug sensitivity by MTT assay as detailed in the Supplementary Materials and Methods. The nature of the interaction between drugs (synergy/antagonism) was assessed at each drug concentration using the Bliss additivity model.23,24
Gene expression analysis
Microarray analysis of gene expression using RNA extracted from patient and xenograft cells was carried out as described in the Supplementary Materials and Methods.
Results
In vivo selection of drug-resistant T-ALL xenograft lines
The xenografts used in this study were derived from diagnosis specimens of T-ALL patients, two of whom relapsed early (<1 year) and succumbed to their disease (ALL-27 and ALL-31, Table 1). The latter patient was highly refractory to treatment, and a sample obtained on day 103 was used to generate xenograft ALL-31b (Table 1). This presented the opportunity to compare experimentally derived and clinically derived drug-resistant phenotypes.
We previously optimized an induction-type regimen of VCR, DEX and ASP (VXL) for pre-clinical ALL studies in NOD/SCID mice.25 To improve the clinical relevance of the model in the current study, we included the anthracycline DNR in the VXL backbone. The maximum tolerated dose of DNR in NOD/SCID mice was 2.5 mg/kg administered i.v. once per week (Supplementary Table 1). At this dose and schedule DNR, delayed disease progression by 8.1 days in the previously characterized T-ALL xenograft ALL-16,17 and when added to the VXL platform (VXLD) extended the progression delay of ALL-31 from 26.4– to 41.0 days (data not shown). Therefore, this dose and schedule of DNR exerted anti-leukemic efficacy in vivo. We next developed protocols for the in vivo selection of drug-resistant xenografts based on the VXLD platform. A 4-week induction schedule was adopted, analogous to the clinical regimen, which clearly delayed disease progression in all four xenografts (Figures 1a–d). The intention was to allow disease reappearance in the peripheral blood and resume cycles of VXLD treatment until the disease progressed through the treatment. Based on tolerability and the proportion of mice with re-emergence of disease, we eventually adopted a protocol consisting of a 4-week block of VXLD, followed at disease re-emergence by a 2-week block of half-dose VXL (Figures 1a–d, and Supplementary Table 2). Re-emerging lines (herein labeled ‘R’) were thus harvested after either one block of therapy (‘VXLD’) or repeated chemotherapy blocks (‘VXLD2’), respectively. Passage-matched controls (labeled ‘C’) were also harvested for each xenograft line.

In vivo drug treatment of T-ALL xenografts. (a) ALL-31, (b) ALL-27, (c) ALL-29 and (d) ALL-33 were treated with either single (VXLD) or multiple (VXLD2) rounds of treatment, or saline (control), to generate lines resistant to multidrug chemotherapy. Acquired drug resistance to single agent ASP (e, f), single agent DNR and VCR (i, j) and single agent DEX, or VXLD combination therapy (g, h) was assessed in ALL-31R (derived from VXLD2-treated ALL-31) and compared with passage-matched ALL-31C, with time course of huCD45+ cells (e, g, i) and survival plots (f, h, j) for the groups of mice in each drug treatment. Baseline engraftment ALL-31C or ALL-31R treated with saline only is indicated in e.
Ex vivo and in vivo assessment of drug resistance in relapsing xenografts
Leukemia cells isolated from in vivo drug-selected xenografts were tested ex vivo against each of the four drugs in VXLD (Supplementary Figure 1). ALL-27R derived from either VXLD or VXLD2 demonstrated increased resistance to DEX, with a trend to higher resistance in the VXLD2 line (Supplementary Figure 1A top panels). Both treatment regimens in ALL-31 were associated with increased resistance to DEX (Supplementary Figure 1A middle panels) and acquired ASP resistance (Supplementary Figure 1A lower panels) compared with the parental line, and again this resistance was more pronounced in ALL-31R derived from the VXLD2 protocol. No acquired resistance to VCR or DNR was observed in ALL-27R and ALL-31R compared with controls (Supplementary Figure 1B). No change in sensitivity to any of the four drugs was observed in ALL-29R and ALL-33R (Supplementary Figure 1C). In summary, DEX and ASP were the main drugs associated with acquired resistance, a phenotype observed in two out of the four xenografts. In each case, the VXLD2 regimen was associated with higher resistance than VXLD, demonstrating the merit of repeated blocks of treatment to establish the model.
To confirm the significance of these ex vivo findings, the drug responses of the VXLD2-treated ALL-31R line were compared in vivo to ALL-31C (Figures 1e–j). The single-agent dosing regimens are detailed in Supplementary Table 1. ALL-31R itself demonstrated accelerated engraftment in the absence of drug compared with ALL-31C (Figure 1e, vehicle), as well as faster leukemic relapse following the treatment with ASP (Figures 1e and f), DEX or VXLD (Figures 1g and h). In vivo resistance to DNR and VCR was not observed (Figures 1i and j). Statistically significant decreases in leukemia progression were observed for DEX (−6.8 days, P=0.0112), ASP (−2.9 days, P=0.0479) and VXLD (−4.6 days, P=0.0026) but not for DNR (1.1 days, P=0.57; Supplementary Table 3). Overall, the drug resistance phenotype of ALL-31R observed from ex vivo studies was supported by the findings from in vivo drug resistance profiling, confirming acquired resistance to both DEX and ASP.
Analysis of genes and pathways associated with acquired drug resistance
To identify biological pathways involved in drug resistance and relapse, we performed gene expression profiling of VXLD treated and controls from each of the xenografts ALL-27, ALL-29, ALL-31 and ALL-33. Volcano plots visually identified transcript clusters with differential gene expression in treated vs control lines, as defined by both adjusted P-value (P<0.05) and absolute fold change (>1.5). Using this approach, both ALL-27R (Figure 2a) and ALL-31R VXLD-treated cells (Figure 2b) demonstrated significant changes in gene expression, but significant differences were not observed in either ALL-29R or ALL-33R (Figure 2c). This finding appears to be consistent with the known clinical status of the patients from whom xenografts ALL-29 and ALL-33 were generated. Both patients remain in long-term remission and their respective xenografts did not show resistance following treatment with either VXLD or VXLD2. The transcript clusters most significantly associated with acquired resistance in ALL-27R and ALL-31R are detailed in Supplementary Tables 4 and 5.

Gene expression analysis of acquired drug resistance in T-ALL xenografts. Volcano plots of differential gene expression (VXLD treated vs passage matched control) for (a) ALL-27R and (b) ALL-31R. (c) Correlation between differences in gene expression and drug resistance phenotype for VXLD-treated xenografts. (d) Gene expression comparison of control or VXLD-treated ALL-31R with ALL-31b (derived from the day103 relapse specimen of same patient). (e) Venn diagram showing overlap of resistance-associated gene expression signatures between ALL-27R and ALL-31R (unadjusted P<0.05 with direction of fold-change taken into account, that is, overlapping genes move in the same direction). (f) Ingenuity Pathway Analysis of resistance-associated gene expression changes affecting ALL-27R and ALL-31R in common (that is, the 399 transcript clusters from Venn diagram intersect) or separately (top 1000 most-significant transcript clusters from either line). Heatmap shows top biological functions, canonical pathways and upstream-network regulators (for example, transcription factors or chemical perturbations) associated with resistance signatures (VXLD-treated vs control). Highlighted pathways are those with a predicted directionality of effect (green, pathway activated in resistant cells; red, pathway downregulated in resistant cells) or networks directly associated with agents used in this study (DEX and SVT, blue highlight). (g) MYC-regulation network associated with acquired resistance in ALL-27R (Ingenuity Pathway Analysis). Colors represent log-fold change (green, expression increased in VXLD-treated xenografts; red, decreased expression in VXLD-treated xenografts; a larger version of this figure can be found in Supplementary Figure 7).
ALL-31 was derived from the diagnosis specimen of a patient who proved to be refractory to treatment, and a biopsy taken at day 103 was used to generate xenograft ALL-31b (Table 1). An analysis of the gene expression profile of ALL-31b demonstrated it to be remarkably similar to that of the VXLD-treated ALL-31R with only four transcript clusters differentially expressed between the two lines (Figure 2d). In contrast, more than 900 transcript clusters were differentially expressed (adjusted P<0.05) when comparing ALL-31b with the saline-treated ALL-31C (Figure 2d). This indicates that the pre-clinical model of induction therapy that we have developed in this study can effectively recapitulate the development of clinical drug resistance.
To identify biological pathways associated with the development of drug resistance, we compared the wider gene expression changes in ALL-27R and ALL-31R using a less stringent statistical cutoff (P<0.05 unadjusted) and observed that although there was a distinct overlap (399 transcript clusters with significant change in expression and consistent directionality), a larger proportion of these responses were unique to each line (Figure 2e). Ingenuity Pathway Analysis of the signatures common and unique to ALL-27R and ALL-31R identified some of the apparent mechanisms underpinning these profiles (Figure 2f). Common to both resistant lines were changes to DNA repair pathways, cell death and survival signaling, and cell cycle regulation with obvious relevance for cellular drug sensitivity. Particularly relevant for the DEX-resistant phenotype observed in both ALL-27R and ALL-31R were pathways involved in lipid biosynthesis (Figure 2f, and Supplementary Figure 2), carbohydrate metabolism and SREBF signaling (sterol regulator-element binding factor, Supplementary Figure 3). We have previously reported that glucocorticoid resistance in T-ALL is associated with a proliferative metabolism and changes in the cholesterol biosynthesis pathway,26, 27, 28 consistent with the findings from the present study. The acquired DEX-resistance of ALL-27R was also strongly associated with gene networks under the control of MYC, MYCN and MAPK (Figures 2f and g), with the direction of these changes predicted to be consistent with an activated status (a larger version of the network shown in Figure 2g can be found in Supplementary Figure 7). These, together with signatures for ERBB2 (Supplementary Figure 4), harvey rat sarcoma viral oncogene homolog, kirsten rat sarcoma viral oncogene homolog and transforming growth factor-β signaling, indicate the general involvement of pathways involved with cell growth and survival in drug-resistant ALL-27R. A network associated with the cellular response to DEX was also highlighted in this analysis (Figure 2f and Supplementary Figure 5). Resistance in ALL-31R was characterized by pathways associated with cytokine signaling (erythropoietin, chemokine (C-C motif) ligand 5, zeta-chain (TCR) associated protein kinase 70kDa, LCK proto-oncogene, Src family tyrosine kinase), nuclear signaling (signal transducer and activator of transcription 2, nuclear transcription factor Y, alpha, histone deacetylase), cholesterol biosynthesis and response networks associated with the drug SVT, a blood-cholesterol lowering agent, see Supplementary Figure 6. As part of these latter networks, upregulation of ASNS (asparagine synthetase) was evident, a notable observation as ALL-31R demonstrated acquired resistance to ASP, for which ASNS upregulation is a known mechanism of resistance.
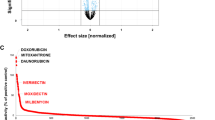
Identification of novel agents to overcome drug resistance
To search for compounds that would be predicted to reverse the resistance phenotypes observed in ALL-27R and ALL-31R, genes significantly associated with acquired resistance (adjusted P-value <0.05) were analyzed using CMap,21,29 which is an approach we have previously used to identify compounds that have cytotoxic synergy in T-ALL.26 Compounds with negative CMap scores would be predicted to antagonize the drug-resistant phenotype under examination. This analysis identified a large number of potential compounds for each of the xenografts, but there was a high degree of overlap in the classes of drugs identified (Table 2). Several of these classes (for example, topoisomerase inhibitors, mammalian target of rapamycin inhibitors and histone deacetylase inhibitors) contain agents that are currently being investigated for their benefit in the treatment of ALL.
Of particular interest to us were drug classes with direct relevance for the alteration in lipid and cholesterol metabolism as this was one of the strongest biological features of resistant xenografts (Figure 2f), namely the HMGCR (3-hydroxy-3-methyl-glutaryl-CoA reductase) inhibitors, peroxisome proliferator-activated receptor γ) agonists and inhibitors of fatty acid β-oxidation (Table 2). HMGCR is one of the rate-limiting enzymes for cholesterol synthesis, whereas peroxisome proliferator-activated receptor γ is a nuclear receptor that regulates fatty acid metabolism, cellular energy and apoptosis,30,31 pathways that have gained a significant amount of interest in recent years as anti-cancer targets.22,30, 31, 32, 33, 34, 35, 36, 37, 38 In addition, transcriptional response to the HMGCR inhibitor SVT was one of the significant networks associated with resistance in ALL-31R (Figure 2f and Supplementary Figure 6). Based on these observations, we selected the HMGCR inhibitor SVT, the peroxisome proliferator-activated receptor γ agonist pioglitazone (PGZ) and the fatty acid β-oxidation inhibitor trimetazidine for further study. We also included the histone deacetylase inhibitor vorinostat (SAHA) as this pathway featured in both the CMap and Ingenuity Pathway analyses (Table 2 and Figure 2f) and we have previously demonstrated the drug to have potential for the reversal of glucocorticoid resistance in pediatric ALL.39
As the Broad Institute originally used cell lines exposed to 10 μM drug concentrations to generate the CMap, we defined an IC50 value of <10 μM as the cutoff for a drug to exhibit single-agent activity. With the exception of SAHA, none of the novel agents demonstrated potent single-agent in vitro efficacy against the parental lines (Supplementary Table 6). The combination of DEX and SVT demonstrated different interaction effects in ALL-27R (Figure 3a) and ALL-31R (Figure 3b), with significant synergy only evident for the latter, consistent with the observation that SVT-response networks and cholesterol metabolism were associated most strongly in this xenograft. The synergy effect was not significant, however, in the ALL-31C control line (see Figure 3e) indicating that this effect was indeed related to the reversal of a resistant phenotype. Unexpectedly, SAHA was antagonistic with DEX in both ALL-27R and ALL-31R, but the effect was milder in ALL-31R (Figures 3c, d and e). Trimetazidine showed no synergy with DEX in ALL-27C/ALL-27R (Figure 3e; trimetazidine not tested in ALL-31), but PGZ demonstrated synergism with DEX in both ALL-31C and ALL-31R (Figure 3e). Synergy of PGZ was also seen in combination with ASP in ALL-31C, but in ALL-31R, it was associated with antagonism (Figure 3e). In summary, of the combinations tested, only SVT showed significant synergy with DEX in any of the resistant xenografts, that being ALL-31R.

Ex vivo drug synergy assessment in T-ALL xenograft lines. The cytotoxicity of the indicated drugs in cells from resistant (VXLD2-treated) xenografts was assessed by MTT assay both as single agents and in combination, using fixed IC50 ratios. A comparison of observed (mean±s.e.m.) and predicted cytotoxic drug responses is shown for (a) ALL-27R (combined DEX+SVT), (b) ALL-31R (combined DEX+SVT), (c) ALL-27R (combined DEX+SAHA) and (d) ALL-31R (combined DEX+SAHA), with deviations from the predicted curve corresponding to antagonistic (less than additive cytotoxic effects) or synergistic (greater than additive cytotoxicity) effects as indicated. (e) The size of the deviation from Bliss additivity across all IC50 ratios was averaged across experiments (n=3 to 5 independent experiments per drug combination) to obtain the net synergy effect over all drug concentrations for that combination (±s.e.m.). Positive scores represent a mean cytotoxic effect greater than that predicted by additive effects alone and thus indicate a net synergistic relationship between the two drugs over all drug concentrations tested (vice versa for antagonism). Significant positive or negative deviation of the mean from zero was assessed by one-tailed t-test, *P<0.05, **P<0.01, ***P<0.001.
In vivo efficacy of SVT in the treatment of drug-resistant T-ALL
We next wished to determine whether the apparent benefit of SVT to overcome resistance in ALL-31R could be translated in vivo. As the identification of SVT as a therapy from gene expression profiling was derived from experiments based on the VXLD protocol, these in vivo studies were designed to test the combination of SVT and VXLD. The maximally tolerated dose for SVT when used in combination with VXLD was 20 mg/kg, and the aim was to determine whether SVT could reverse or delay leukemia relapse induced by a 4-week multidrug induction regimen.
SVT alone induced no significant delay of ALL-31R engraftment to the spleen, BM or peripheral blood (Figures 4a–c), and we observed no in vivo synergy of SVT in combination with VXLD, with almost identical patterns of engraftment (Figures 4a–c). SVT as a single agent did not significantly increase mouse event-free survival, whereas VXLD treatment significantly delayed the progression of ALL-31R by 33.4 days compared with vehicle-treated mice (Figures 4d and e). The combination of SVT and VXLD caused no significant delay in leukemia progression compared with VXLD alone. Thus, despite the findings from gene expression, in vitro and ex vivo experiments, use of SVT in vivo at this dose was unable to sensitize leukemia cells to treatment with VXLD.

Efficacy of SVT (20 mg/kg) for treatment of drug-resistant T-ALL. (a–c) Engraftment of ALL-31R (% Hu CD45+ cells) over time in (a) spleen, (b) bone marrow or (c) peripheral blood in mice treated with vehicle (black solid line), SVT (gray dotted line), VXLD (gray solid line) or VXLD+SVT (black dotted line). (d, e) Effect of vehicle (black solid line), SVT (gray dotted line), VXLD (gray solid line) and SVT+VXLD (black dotted line) on survival (d) and the time course for the appearance of human CD45+ cells in peripheral blood (e).
Discussion
In this study, we have reported for the first time the development of a powerful pre-clinical in vivo model of ALL induction therapy that allows for the investigation of mechanisms of resistance. The data indicate that the model accurately recapitulates the in vivo development of resistance as demonstrated by the comparison of drug-resistant xenografts derived experimentally (ALL-31R) vs clinically (ALL-31b, from a therapy-resistant patient). The differences in gene expression observed between diagnosis and relapse, or parental and drug-treated xenograft lines, may reflect phenotypic changes of the leukemia cells themselves, the selection and out-growth of resistant subpopulations present at the time of diagnosis,40 or a combination of both mechanisms.41,42 Under either scenario, the model developed here appears to represent a clinically relevant model of resistance to induction therapy. Using this approach, we have identified biological signatures associated with the development of resistance in vivo and have ascertained, as one might expect, that patterns of resistance are different among tumors derived from individual patients. In two of the four leukemia lines tested, no drug resistance emerged after repeated drug treatment, and this correlates with the clinical course of the patients in question as these individuals remain in clinical remission. However, the two other leukemia lines (ALL-27R and ALL-31R) developed drug-resistant phenotypes associated with distinct changes in gene expression, including a prominent activation of MYC and MAPK signaling in one case, and a deregulation of cytokine and nuclear signaling networks in the other. Importantly, changes to lipid and carbohydrate metabolism featured in both resistant lines, an observation that led us to focus on a number of agents that modulate these pathways as a proof-of-concept approach to overcome resistance in ALL.
The inclusion of SVT in ALL therapy regimens is an attractive concept as the drug is generally well tolerated (it is commonly used as an anti-hypercholesterolemia agent) and could potentially alleviate morbidity associated with osteonecrosis, something that affects up to 70% of ALL patients, and for which high levels of cholesterol and treatment with steroids are known risk factors.43 Although statins have been demonstrated to have anticancer effects, studies of their potential of chemoresistance reversal in ALL have never been reported.35,44 However, despite the apparent promise of SVT from the gene expression data and its successful assessment ex vivo, these findings did not translate in vivo.
Our ex vivo fixed ratio combination cytotoxicity assays that validated SVT as a potential resistance-reversing drug required continuous exposure to 10–40 μM SVT for 48 h (Figure 3b and Supplementary Table 6). In a recent study carried out in mice administered with 10 mg/kg SVT via oral gavage,45 the highest achievable plasma concentration (<3 μM) was considerably less than the minimum SVT concentration used in our study to achieve synergy. It may not be surprising, therefore, that daily × 5 dosing of SVT at 20 mg/kg is unable to recapitulate the continuous exposure to 10–40 μM SVT for 48 h used in our assays. Although a number of studies have now successfully recapitulated in vitro CMap findings in vivo,21 many published reports stop at the stage of testing their drug-leads in vitro.20,46 Had we not proceeded to test SVT in vivo, we too would have concluded a clinical benefit of SVT in combination with VXLD. It is clear that in using CMap for drug repositioning or drug discovery it is very important to carefully assess the appropriateness of the biological context for the model, and to validate any findings in vivo.
Recently, Hartwell et al.47 used a completely different approach of a high-throughput screen in a co-culture system and identified the cholesterol lowering drug, Lovostatin, which had a cell-autonomous activity against AML cells. However, an on-target effect of Lovastatin was limited to ex vivo analysis because of the expected low concentration to be achieved in BM for their in vivo study. Our data using T-ALL cells are complementary, especially in the context of completely different experimental approaches to identify a similar class of drugs. Failure to see an in vivo effect of SVT in our own study is likely related to the concentration achievable in the BM in vivo within the limits of toxicity, and is thus likely to be a major important factor in the potential translation of this therapeutic approach into the clinic.
It remains possible that a benefit of SVT in combination with DEX as a single agent (as opposed to the more cytotoxic VXLD regimen) could be achievable if this was to be tested in vivo, however, the issue of SVT dosing would remain the same. We have not tested PGZ in vivo in this study, however, as an alternative modulator of lipid and cholesterol metabolism; it remains a potential candidate for further therapeutic testing in ALL.
The observation that DEX and SAHA were antagonistic in this study is surprising, given that previous studies, including those from our own groups39 have suggested that this combination may be of benefit in T-ALL. Therefore, these results will require corroboration in a larger number of T-ALL xenografts. In conclusion, this study has resulted in the development of a clinically relevant in vivo model of ALL induction therapy that can be used to interrogate mechanisms of drug resistance. We are now extending this study to larger numbers of ALL xenografts to capture a greater diversity of relapsing profiles and identify alternative therapeutic approaches.
References
Kaatsch P . Epidemiology of childhood cancer. Cancer Treat Rev 2010; 36: 277–285.
Lo Nigro L . Biology of childhood acute lymphoblastic leukemia. J Pediatr Hematol Oncol 2013; 35: 245–252.
Pui CH, Mullighan CG, Evans WE, Relling MV . Pediatric acute lymphoblastic leukemia: where are we going and how do we get there? Blood 2012; 120: 1165–1174.
Bhadri VA, Trahair TN, Lock RB . Glucocorticoid resistance in paediatric acute lymphoblastic leukaemia. J Paediatr Child Health 2012; 48: 634–640.
Pui CH, Evans WE . Treatment of acute lymphoblastic leukemia. N Engl J Med 2006; 354: 166–178.
Dordelmann M, Reiter A, Borkhardt A, Ludwig WD, Gotz N, Viehmann S et al. Prednisone response is the strongest predictor of treatment outcome in infant acute lymphoblastic leukemia. Blood 1999; 94: 1209–1217.
Den Boer ML, Harms DO, Pieters R, Kazemier KM, Gobel U, Korholz D et al. Patient stratification based on prednisolone-vincristine-asparaginase resistance profiles in children with acute lymphoblastic leukemia. J Clin Oncol 2003; 21: 3262–3268.
Kaspers GJ, Veerman AJ, Pieters R, Van Zantwijk CH, Smets LA, Van Wering ER et al. In vitro cellular drug resistance and prognosis in newly diagnosed childhood acute lymphoblastic leukemia. Blood 1997; 90: 2723–2729.
Locatelli F, Schrappe M, Bernardo ME, Rutella S . How I treat relapsed childhood acute lymphoblastic leukemia. Blood 2012; 120: 2807–2816.
Marshall GM, Dalla Pozza L, Sutton R, Ng A, de Groot-Kruseman HA, van der Velden VH et al. High-risk childhood acute lymphoblastic leukemia in first remission treated with novel intensive chemotherapy and allogeneic transplantation. Leukemia 2013; 27: 1497–1503.
Bailey LC, Lange BJ, Rheingold SR, Bunin NJ . Bone-marrow relapse in paediatric acute lymphoblastic leukaemia. Lancet Oncol 2008; 9: 873–883.
Kaspers GJ, Wijnands JJ, Hartmann R, Huismans L, Loonen AH, Stackelberg A et al. Immunophenotypic cell lineage and in vitro cellular drug resistance in childhood relapsed acute lymphoblastic leukaemia. Eur J Cancer 2005; 41: 1300–1303.
Klumper E, Pieters R, Veerman AJ, Huismans DR, Loonen AH, Hahlen K et al. In vitro cellular drug resistance in children with relapsed/refractory acute lymphoblastic leukemia. Blood 1995; 86: 3861–3868.
Tentler JJ, Tan AC, Weekes CD, Jimeno A, Leong S, Pitts TM et al. Patient-derived tumour xenografts as models for oncology drug development. Nat Rev Clin Oncol 2012; 9: 338–350.
Macor P, Secco E, Zorzet S, Tripodo C, Celeghini C, Tedesco F . An update on the xenograft and mouse models suitable for investigating new therapeutic compounds for the treatment of B-cell malignancies. Curr Pharm Des 2008; 14: 2023–2039.
Lock RB, Liem N, Farnsworth ML, Milross CG, Xue C, Tajbakhsh M et al. The nonobese diabetic/severe combined immunodeficient (NOD/SCID) mouse model of childhood acute lymphoblastic leukemia reveals intrinsic differences in biologic characteristics at diagnosis and relapse. Blood 2002; 99: 4100–4108.
Liem NL, Papa RA, Milross CG, Schmid MA, Tajbakhsh M, Choi S et al. Characterization of childhood acute lymphoblastic leukemia xenograft models for the preclinical evaluation of new therapies. Blood 2004; 103: 3905–3914.
Bhadri VA, Cowley MJ, Kaplan W, Trahair TN, Lock RB . Evaluation of the NOD/SCID xenograft model for glucocorticoid-regulated gene expression in childhood B-cell precursor acute lymphoblastic leukemia. BMC Genomics 2011; 12: 565.
Houghton PJ, Morton CL, Tucker C, Payne D, Favours E, Cole C et al. The pediatric preclinical testing program: description of models and early testing results. Pediatr Blood Cancer 2007; 49: 928–940.
Wei G, Twomey D, Lamb J, Schlis K, Agarwal J, Stam RW et al. Gene expression-based chemical genomics identifies rapamycin as a modulator of MCL1 and glucocorticoid resistance. Cancer Cell 2006; 10: 349–351.
Qu XA, Rajpal DK . Applications of Connectivity Map in drug discovery and development. Drug Discov Today 2012; 17: 1289–1298.
Wong WW, Dimitroulakos J, Minden MD, Penn LZ . HMG-CoA reductase inhibitors and the malignant cell: the statin family of drugs as triggers of tumor-specific apoptosis. Leukemia 2002; 16: 508–519.
Borisy AA, Elliott PJ, Hurst NW, Lee MS, Lehar J, Price ER et al. Systematic discovery of multicomponent therapeutics. Proc Natl Acad Sci U S A 2003; 100: 7977–7982.
Winter GE, Rix U, Carlson SM, Gleixner KV, Grebien F, Gridling M et al. Systems-pharmacology dissection of a drug synergy in imatinib-resistant CML. Nat Chem Biol 2013; 8: 905–912.
Szymanska B, Wilczynska-Kalak U, Kang MH, Liem NLM, Carol H, Boehm I et al. Pharmacokinetic modeling of an induction regimen for in vivo combined testing of novel drugs against pediatric acute lymphoblastic leukemia xenografts. PLoS ONE 2012; 7: e33894.
Beesley AH, Firth MJ, Ford J, Weller RE, Freitas JR, Perera KU et al. Glucocorticoid resistance in T-lineage acute lymphoblastic leukaemia is associated with a proliferative metabolism. Br J Cancer 2009; 100: 1926–1936.
Beesley AH, Rampellini JL, Palmer ML, Heng JY, Samuels AL, Firth MJ et al. Influence of wild-type MLL on glucocorticoid sensitivity and response to DNA-damage in pediatric acute lymphoblastic leukemia. Mol Cancer 2010; 9: 284.
Beesley AH, Firth MJ, Anderson D, Samuels AL, Ford J, Kees UR . Drug-gene modeling in pediatric T-cell acute lymphoblastic leukemia highlights importance of 6-mercaptopurine for outcome. Cancer Res 2013; 73: 2749–2759.
Lamb J, Crawford ED, Peck D, Modell JW, Blat IC, Wrobel MJ et al. The Connectivity Map: using gene-expression signatures to connect small molecules, genes, and disease. Science 2006; 313: 1929–1935.
Konopleva M, Andreeff M . Role of peroxisome proliferator-activated receptor-gamma in hematologic malignancies. Curr Opin Hematol 2002; 9: 294–302.
Koeffler HP . Peroxisome proliferator-activated receptor gamma and cancers. Clin Cancer Res 2003; 9: 1–9.
Hindler K, Cleeland CS, Rivera E . Collard CD. The role of statins in cancer therapy. Oncologist 2006; 11: 306–315.
Andela VB, Pirri M, Schwarz EM, Puzas EJ, O'Keefe RJ, Rosenblatt JD et al. The mevalonate synthesis pathway as a therapeutic target in cancer. Clin Orthop Relat Res 2003, S59–S66.
Infante E, Heasman SJ, Ridley AJ . Statins inhibit T-acute lymphoblastic leukemia cell adhesion and migration through Rap1b. J Leukocyte Biol 2011; 89: 577–586.
Li HY, Appelbaum FR, Willman CL, Zager RA, Banker DE . Cholesterol-modulating agents kill acute myeloid leukemia cells and sensitize them to therapeutics by blocking adaptive cholesterol responses. Blood 2003; 101: 3628–3634.
Calabro A, Tai J, Allen SL, Budman DR . In-vitro synergism of m-TOR inhibitors, statins, and classical chemotherapy: potential implications in acute leukemia. Anticancer Drugs 2008; 19: 705–712.
Andela VB, Altuwaijri S, Wood J, Rosier RN . Inhibition of beta-oxidative respiration is a therapeutic window associated with the cancer chemo-preventive activity of PPARgamma agonists. FEBS Lett 2005; 579: 1765–1769.
Samudio I, Harmancey R, Fiegl M, Kantarjian H, Konopleva M, Korchin B et al. Pharmacologic inhibition of fatty acid oxidation sensitizes human leukemia cells to apoptosis induction. J Clin Invest 2010; 120: 142–156.
Bachmann PS, Piazza RG, Janes ME, Wong NC, Davies C, Mogavero A et al. Epigenetic silencing of BIM in glucocorticoid poor-responsive pediatric acute lymphoblastic leukemia, and its reversal by histone deacetylase inhibition. Blood 2010; 116: 3013–3022.
Anderson K, Lutz C, van Delft FW, Bateman CM, Guo Y, Colman SM et al. Genetic variegation of clonal architecture and propagating cells in leukaemia. Nature 2011; 469: 356–361.
Clappier E, Gerby B, Sigaux F, Delord M, Touzri F, Hernandez L et al. Clonal selection in xenografted human T cell acute lymphoblastic leukemia recapitulates gain of malignancy at relapse. J Exp Med 2011; 208: 653–661.
Choi S, Henderson MJ, Kwan E, Beesley AH, Sutton R, Bahar AY et al. Relapse in children with acute lymphoblastic leukemia involving selection of a preexisting drug-resistant subclone. Blood 2007; 110: 632–639.
Kawedia JD, Kaste SC, Pei D, Panetta JC, Cai X, Cheng C et al. Pharmacokinetic, pharmacodynamic, and pharmacogenetic determinants of osteonecrosis in children with acute lymphoblastic leukemia. Blood 2011; 117: 2340–2347.
Chan KKW, Oza AM, Siu LL . The statins as anticancer agents. Clin Cancer Res 2003; 9: 10–19.
van de Steeg E, Kleemann R, Jansen HT, van Duyvenvoorde W, Offerman EH, Wortelboer HM et al. Combined analysis of pharmacokinetic and efficacy data of preclinical studies with statins markedly improves translation of drug efficacy to human trials. J Pharmacol Exp Ther 2013; 347: 635–644.
Sanda T, Li X, Gutierrez A, Ahn Y, Neuberg DS, O'Neil J et al. Interconnecting molecular pathways in the pathogenesis and drug sensitivity of T-cell acute lymphoblastic leukemia. Blood 2010; 115: 1735–1745.
Hartwell KA, Miller PG, Mukherjee S, Kahn AR, Stewart AL, Logan DJ et al. Niche-based screening identifies small-molecule inhibitors of leukemia stem cells. Nat Chem Biol 2013; 9: 840–848.
Acknowledgements
This study was supported by National Health and Medical Research Council Projects Grants ID513765 and ID1011499, and Research Fellowship (RBL). We thank the patients and staff of Sydney Children’s Hospital for the provision of ALL biopsies. Children’s Cancer Institute Australia for Medical Research is affiliated with the University of New South Wales and the Sydney Children’s Hospitals Network.
Author Contributions
ALS, AHB, URK and RBL designed the study; ALS, AHB, BDY, RAP and DA carried out the experiments and analyzed the data; RS, GMM and CHC provided patient biopsies. All authors contributed to the manuscript.
Author information
Authors and Affiliations
Corresponding author
Ethics declarations
Competing interests
The authors declare no conflict of interest.
Additional information
Supplementary Information accompanies this paper on Blood Cancer Journal website
Supplementary information
Rights and permissions
This work is licensed under a Creative Commons Attribution-NonCommercial-NoDerivs 4.0 International License. The images or other third party material in this article are included in the article’s Creative Commons license, unless indicated otherwise in the credit line; if the material is not included under the Creative Commons license, users will need to obtain permission from the license holder to reproduce the material. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-nd/4.0/
About this article

Cite this article
Samuels, A., Beesley, A., Yadav, B. et al. A pre-clinical model of resistance to induction therapy in pediatric acute lymphoblastic leukemia. Blood Cancer Journal 4, e232 (2014). https://doi.org/10.1038/bcj.2014.52
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/bcj.2014.52
This article is cited by
-
Integrated multi-omics analyses reveal homology-directed repair pathway as a unique dependency in near-haploid leukemia
Blood Cancer Journal (2023)
-
Central nervous system involvement in childhood acute lymphoblastic leukemia is linked to upregulation of cholesterol biosynthetic pathways
Leukemia (2022)
-
Chemotherapy induces canalization of cell state in childhood B-cell precursor acute lymphoblastic leukemia
Nature Cancer (2021)
-
Metabolic reprogramming of acute lymphoblastic leukemia cells in response to glucocorticoid treatment
Cell Death & Disease (2018)
-
Drug-induced amino acid deprivation as strategy for cancer therapy
Journal of Hematology & Oncology (2017)
