
Abstract
Aims
To review the ocular manifestations of crush head injuries in children.
Methods
Retrospective clinical and pathological reviews. Group 1: A total of 16 children admitted with crush head injuries from television tip over. Group 2: Nine autopsy findings in crush head injury.
Results
Group 1: A total of 11 children had fundus examination: three by neurosurgeons, eight by ophthalmologists. Scattered posterior pole preretinal and blot haemorrhages extending to mid equator region observed in one child. No evidence of traumatic retinoschisis or retinal folds in any patient. Group 2: All with multiple skull fractures and six with subdural haemorrhage. Posterior pole retinal haemorrhages in four children, extending to the ora serrata in one after motor vehicle accident. No child had retinal folds. Subinternal limiting membrane haemorrhages in three children. Optic nerve sheath haemorrhage in three children.
Conclusions
Intraretinal and preretinal haemorrhages, predominantly in the posterior pole, can occur in crush injury to the paediatric head. Haemorrhage under the internal limiting membrane or extending to the ora serrata were only seen in situations where crush injury was part of a fatal trauma scenario related to motor vehicles. Retinal folds and the typical macular retinoschisis associated with abusive head injury were not observed.
Similar content being viewed by others

Introduction
Crush injuries involve the application of force over a relatively prolonged interval (more than 200 ms) and wide area as compared to simple blunt impact. 1, 2 The forces involved usually include both static and dynamic components. Static loading of the head occurs when the head is stationary and pinned against a rigid structure. Dynamic loading results from sudden rapid movement of the head for a brief period of time.3 In most cases of crush injuries, the static loading is considered to be a greater factor than the dynamic force.2, 4
Some examples of paediatric crush injuries include children knocked to the ground by a toppling television (TV). The crushing weight of the object compressing the child between the heavy object and the ground is a greater factor in the injury than the dynamic force involved in the child falling and impacting the ground.5 Likewise, children whose heads are run over by a vehicle, are first thrown to the ground (dynamic load), and then compressed between the vehicle tyre and the road (static load).6
A recent case report suggested that a TV tip over crush injury to the head of an infant can result in bilateral extensive retinal haemorrhages extending from the posterior pole to the ora serrata affecting the preretinal, intraretinal and subretinal layers with circumlinear perimacular retinal folds.7 Although no other reports of extensive ocular injuries associated with crush injuries of the head in children have been identified in the literature, most studies did not include report of full ocular examination.1, 2, 5, 6, 8, 9 A retrospective clinical and pathological review was conducted to study the ocular manifestations of paediatric crush injury of the head.
Materials and methods
Group 1
Review of the records of The Hospital for Sick Children (HSC) from 1992 to 2002 identified 16 admissions for head injury from falling TVs. The data collected from these 16 records included age, sex, extent of injury, site of injury, surgical intervention, length of hospital stay, follow–up, and clinical outcome. When an ocular examination was conducted, the specialty service that performed that examination was noted and the results were recorded with particular attention to the presence of blunt eye injury and fundus examination. Data were entered and analysed using the data analysis module from Microsoft Excel 7.0 (Redmond, WA). This study was approved by The Hospital for Sick Children, Research Ethics Board.
Group 2
Of approximately 400 child deaths investigated at the Dallas County Medical Examiner's Office from 1982 to 1989, 169 were prospectively studied. Selection depended on the prosectors' willingness to participate in the ocular study. History, autopsy findings, and ocular findings were gathered and reviewed. The ocular findings of 169 children have been previously reported.9, 10 The 169 deaths included diagnoses of child abuse, suspected child abuse, accidental trauma, and non-traumatic death. The ocular findings in those cases in which there was a crush injury to the head are reported. Complete autopsies were performed on all cases in this subgroup.9
Results
Group 1
The findings in this group are detailed in Table 1. The neurosurgical manifestations of this group have been reported in more detail elsewhere (in press). Of the 16 children admitted to HSC, 11 were boys. The mean age of the group was 48.8 months (range 12–120). The dimensions of the TV screen were between 45 and 80 cm and the height of the TV fall between 1 and 2 m. On presentation to the emergency room, one child had a fixed dilated pupil and one complained of double vision. Blood was noted in the auditory canal in three patients, a mild facial weakness was noted in one child, and depressed level of consciousness was observed in three patients. Only three children required a neurosurgical intervention. These interventions included frontal craniotomy and suturing of a dural laceration in one patient, elevation of the skull fracture in one patient and temporal craniectomy and evacuation of a temporal clot from a subdural haemorrhage in another patient. The mean duration of stay in the hospital was 10 days (range 2–39). No child died. In all, 11 children had fundus examinations: three by the attending neurosurgeon and eight by a consulting ophthalmologist. The timing of the eye examination was within the first 48 h following admission in eight children.
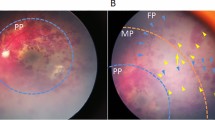
Multiple preretinal and blot haemorrhages located in the posterior pole and extending to the mid equator were observed in one child. This was a 10-year-old boy who presented with biparietal skull fracture, subdural hematoma along the falx and in the frontal convexities after a 63 cm TV fall. His coagulation profile was normal and he had an uneventful recovery. There was no evidence of traumatic retinoschisis or retinal folds in any patient.
Group 2
The findings in these patients are detailed in Table 2. Nine of the 169 children died as a result of crush injuries. Four were boys. The mean age was 21.1 months (range 2–56). There was a history of crush injury in each patient. Eight had multiple skull fractures and six had subdural haemorrhage. Ocular findings include retinal haemorrhages in four children. These were confined to the posterior pole in three. In one, the retinal haemorrhages were scattered diffusely out to the ora serrata. The group with retinal haemorrhages included a pedestrian run over by a motor vehicle, two children who fell out of a car, which then rolled over the children's heads, and an unrestrained passenger in a motor vehicle collision. The latter was the only child with retinal haemorrhages at the ora serrata. No child had retinal folds. Subinternal limiting membrane haemorrhages (SILMH) were observed in three children. All were small, focal elevations of the internal limiting membrane. These foci were present to the mid equator in all three and nearly to the ora serrata in one of the three. Optic nerve sheath haemorrhage was seen in three children all of whom also had subdural haemorrhages. No child had retinal folds or retinoschisis.
Discussion
Crush injuries to the head are the tenth most common cause of injury in children under 9-years old.11 These injuries result from mechanical loading of the head by static forces, applied relatively slowly (greater than 200 ms) over a large area, causing deformation of the cranium.1, 2 However, the injuries are rarely pure and there is often a dynamic component owing to impact of the moving head usually prior to the crush.12 The static loading is often considered a greater factor than the dynamic force. Crush injuries may result in less severe neurological damage and better outcome.4, 13
Serious injury and death can occur when a TV topples from an elevated location in the home. It is estimated that a minimum of approximately 10 children die each year in the United States from such injuries.5 Several physical properties increase the risk of severe injury from toppling TV sets. Conventional television sets utilize cathode ray vacuum tubes having a rugged glass shield fused to or incorporated in their phosphor-bearing front screen. The part of the set closest to the viewer is typically the heavier. The weight increases dramatically with larger screen sizes and the centre of gravity moves forward toward the screen. Television stands and entertainment centres originally designed for smaller sets may be used inappropriately for new, larger TVs and may not be adequate to prevent the set from falling when jostled. The combination of large TV sets and inadequate support may present a significant danger for children, especially toddlers who may attempt to reach up to touch the screen controls.
Crush injury of the head commonly presents with multiple fractures through the cranial base, facial fractures, and cranial nerve palsies.13 Although the medical literature addresses outcome after crush injuries to the head, only one study specifically describes ocular examination findings.1, 2, 5, 6, 8, 9 Duhaime et al1 reported a series of seven crush injuries in young children. All had massive soft tissue swelling of the face with associated orbital fracture in five, cranial nerve damage in four and otorrhea in one. An ophthalmology consultation was done on all patients and although the paper does not specifically report the results of the retinal examination, other ocular abnormalities are reported and there is no mention made of retinal haemorrhages being found. Prasad et al2 studied eight children less than 3-years old with crush head injuries. Five had been run over by cars and three were victims of a TV falling on to their heads from heights of less than approximately 1 m. All children sustained extraaxial haemorrhages and cerebral contusions associated with complicated skull fractures. The systemic injuries include otorrhea in four, pneumocephalus in three, cranial nerve palsy in three, cerebellar contusion/haemorrhage in two, pneumothorax in one, and spleen hematoma in one child. There is no mention of eye examination or any eye findings apart from orbital fracture in one child.2 In a study by DiScala et al on the outcome of TV sets toppling onto toddlers, crush head injury was observed in 68%. The injuries reported were not trivial and 2.7% died from massive intracranial haemorrhage. There was no mention of eye findings.
In our study of 16 TV tip over crush injuries to the head, only one, a 10-year old boy, was found to have retinal haemorrhage: bilateral scattered intra- and preretinal haemorrhages posterior to the equator. In our autopsy series, four children were found to have retinal haemorrhages all of whom received their head crushes as part of a motor vehicle trauma. The retinal haemorrhages were confined to the posterior pole in three. In only one did scattered haemorrhages extend out to the ora serrata. Three were found to have SILM. Optic nerve sheath haemorrhages were documented in three children all of whom had subdural haemorrhage of the brain. No child in either group had retinal folds or the typical macular traumatic retinoschisis previously described in abusive head injury (Shaken Baby syndrome).14, 15
In a recent single case report, Lantz et al7 describe a 14-month-old boy who was the victim of an alleged fatal TV tip over. His cranial computed tomographic scan showed diffuse cerebral edema with subdural blood overlying the frontal convexities and layering along the falx cerebri, a left-sided skull fracture adjacent to a widely diastatic coronal suture and cerebral contusion beneath the fracture. The child had severe, extensive, and almost confluent bilateral intraretinal haemorrhages, preretinal haemorrhages, subretinal haemorrhages, and perimacular circumlinear retinal folds. The haemorrhages extended to 360° to the ora serrata. Although the authors state that the child had retinoschisis, one of the authors of our paper (AVL) has reviewed the original histology images and believes that true splitting of the retina is not present.
This case creates a quandary: why are the retinal findings of Lantz et al7 such a dramatic departure from what has previously been reported in the literature and what we have found in our own study? One possible explanation is that the child was not only a victim of a TV tip over but also a victim of other neurotrauma. The investigative team did an extremely thorough home scene investigation including replication of the tip over using a weight equal to that of the child and the father's history remained consistent, unlike the changing history which often characterizes child abuse. The event was witnessed only by a toddler sibling. Yet, the child did not have some of the typical injuries of head crush trauma such as orbital fracture, multiple skull fracture, hemotympanum, and cranial nerve palsy.1, 2, 13 The authors do not report the results of cervical neck dissection,7 which is a crucial element of the forensic evaluation. Certainly his retinopathy was much more consistent with the retinal haemorrhages that characterize Shaken Baby syndrome.14, 16, 17 However, the perimacular folds were a bit atypical for Shaken Baby syndrome in that they had a much more angulated apex, although this can occasionally be seen at autopsy from a collapsed retinoschisis cavity.18
Another possible explanation for the findings of Lantz et al7 may be that the child or the injury itself occurred in the presence of some unique factor that predisposed the child to the haemorrhagic retinopathy may have been present.19 Although the child was not described as having a significant coagulopathy, perhaps the child had one or more conditions influencing coagulation such as thrombophilic factors,19 subclinical vitamin C deficiency,20 or a collagen disorder.21 No evaluation was done for these disorders. Lastly, we must consider the possibility that crush injury can cause the retinal findings described by Lantz et al7 and would have been eventually observed had our sample size been larger.
Retinal haemorrhages are well recognized, although uncommon, in accidental major head trauma.22 When retinal haemorrhages occur after accidental head injury, they are usually intraretinal or preretinal and posterior to the equator as seen in all but one of our patients with crush injuries. In extremely severe accidental trauma, particularly when there is repeated acceleration–deceleration as in motor vehicle roll over, a more severe haemorrhagic retinopathy, including extension to the ora serrata, can be seen (J Kivlin, personal communication). Haemorrhaging at the ora serrata in infants has otherwise been shown to be statistically more common in Shaken Baby syndrome.14, 23, 24 In children, owing to the firm adhesion between the paediatric vitreous and the posterior retina, violent shaking of the vitreous can cause traction on the retina, with splitting of the retinal layers and accumulation of blood in the resultant schisis cavity. Traumatic retinoschisis, may be either deep to the nerve fiber layer or superficial (involving only the internal limiting membrane). The recognition of traumatic retinoschisis is extremely important. It had been suggested that the lesion is diagnostic of shaking.18 The same authors state, the best way to confirm this assertion is to study a series of eyes taken from children who sustained accidental (not deliberate) direct head trauma.'18
Neither retinoschisis nor paramacular lines or folds were seen in our victims of accidental head crush. We cannot think of a satisfactory pathophysiological mechanism by which a crush injury could result in these findings or the lesions seen in the child described by Lantz et al.7 In our autopsy series we did observe small focal areas of blood beneath the internal limiting membrane (ILM) without folds or hypopigmentation. We suspect the elevation of the ILM may have occurred by very small, focal blood accumulation. It is also possible that the eye, like the brain, could be subject to differential shearing forces as a result of the crush resulting in small areas of focal vitreous traction with tension on the ILM. We cannot rule out the possibility that a larger sample size would reveal other ocular findings not noted here. Our cases of crush head injuries owing to TV tip overs were not investigated for possible abuse, which might be considered in a child with retinal haemorrhages. In our autopsy series, the time between injury and death may have been long enough in one case for retinal haemorrhages to have cleared and therefore be unknown to us. However, retinoschisis, paramacular folds, and extensive retinal haemorrhaging would not likely have resolved in that time period. In the TV tip over group, three children had their eye examination done by a non-ophthalmologist. We do not know if the pupil was dilated or not during that examination, but the instrumentation available to the neurosurgeon (the direct ophthalmoscope) by definition would limit the ability to assess the retina. We have previously studied the accuracy of non-ophthalmologists in examining the retina for haemorrhages in shaken babies and found a remarkably good success rate although false positives and false negatives are known to occur.25 In our experience, the non-ophthalmologists had an 87% success rate in correctly determining if retinal haemorrhage was present or absent.25 However, non-ophthalmologists used the term ‘retinal haemorrhage’ generically and did not further describe the number, type, or distribution pattern of retinal haemorrhages they might see. Our three fundus examinations by attending neurosurgeons were documented as normal and none were subsequently examined by an ophthalmologist.
We conclude that intraretinal and preretinal haemorrhages, predominantly in the posterior pole, and not extending beyond the equator, can occasionally occur in the unique situation of crush injury to the paediatric head. When forces at the level of a motor vehicle accident are involved, the haemorrhages can occasionally extend to the ora and focal subinternal limiting haemorrhage may be seen. However, the presence of severe haemorrhagic retinopathy, retinoschisis or perimacular folds similar to that seen in Shaken Baby syndrome were not seen. Before attributing retinal haemorrhages or perimacular folds to a crush injury, as opposed to inflicted neurotrauma, there must be history and physical findings consistent with a crush mechanism, and meticulous investigation must be undertaken.
References
Duhaime AC, Eppley M, Margulies S, Heher KL, Bartlett SP . Crush injuries to the head in children. Neurosurgery 1995; 37: 401–406.
Prasad MR, Ewing-Cobbs L, Baumgarter J . Crush head injuries in infants and young children: neurologic and neuropsychologic sequelae. J Child Neurol 1999; 14: 496–501.
Gennarelli TA, Meaney DF . Mechanisms of primary head injury. In: Wilkins RH, Rengachary SS (eds) Neurosurgery. McGraw-Hill: New York, NY, 1996 pp 2611–2622.
Holbourn AHS . Mechanics of head injuries. Lancet 1943; 9: 438–441.
DiScala C, Barthel M, Sege R . Outcomes from television sets toppling onto toddlers. Arch Pediatr Adolesc Med 2001; 155: 145–148.
Partrick DA, Bensard DD, Moore EE, Partington MD, Karrer FM . Driveway crush injuries in young children: a highly lethal devastating and potentially preventable event. J Pediatr Surg 1998; 33: 1712–1715.
Lantz PE, Sinal SH, Stanton CA, Weaver Jr RG . Perimacular retinal folds from childhood head trauma. BMJ 2004; 328: 754–756.
Silen ML, Kokoska ER, Fendya DG, Kurkchubasche AG, Weber TR, Tracy TF . Rollover injuries in residential driveways: age-related patterns of injury. Pediatrics 1999; 104: e7.
Gilliland MG, Luckenbackh MW, Chenier TC . Systemic and ocular findings in 169 prospectively studied child deaths: retinal haemorrhages usually mean child abuse. Forensic Sci Int 1994; 16 (68): 117–132.
Gilliland MG, Luckenbackh MW . Are retinal hemorrhages found after resuscitation attempts? A study of the eyes of 169 children. Am J Forensic Med Pathol 1993; 14: 187–192.
Spady DW, Saunders DL, Schopflocher DP, Svenson LW . Patterns of injury in children: a population based approach. Pediatrics 2004; 113: 522–529.
Russell WR, Schiller F . Crushing injuries to the skull: clinical and experimental observations. J Neurol Neurosurg Psychiat 1949; 12: 52–61.
Tortosa JG, Poza MP . Crush injuries to the head. Neurosurgery 1996; 39: 877–878.
Levin AV . Retinal hemorrhages and child abuse. In: David TJ (ed) Recent Advances in Pediatrics, no. 18. Churchill Livingstone: London, 2000 pp 151–219.
Greenwald MJ, Weiss A, Oesterle CS, Friendly DS . Traumatic retinoschisis in battered babies. Ophthalmology 1986; 93: 618–625.
Kivlin JD, Simons KB, Lazoritz S, Ruttum MS . Shaken baby syndrome. Ophthalmology 2000; 107: 1246–1254.
Elner SG, Elner VM, Arnall M, Albert DM . Ocular and associated systemic findings in suspected child abuse. Arch Ophthalmol 1990; 108: 1094–1101.
Massicotte SJ, Folberg R, Torczynski E, Gilliland MG, Luckenbach MW . Vitreoretinaltraction and perimacular retinal folds in the eyes of deliberately traumatized children. Ophthalmology 1991; 98 (7): 1124–1127.
Seligsohn U, Lubetsky A . Genetic susceptibility to venous thrombosis. N Engl J Med 2001; 344: 1222–1231.
Johnston CS, Thompson MS . Vitamin C status of an outpatient population. J Am Coll Nutr 1998; 173: 66–70.
Ganesh A, Jenny C, Geyer J, Shouldice M, Levin AV . Retinal hemorrhages in type I osteogenesis imperfecta following minor trauma. Ophthalmology 2004; 111: 1428–1431.
Buys Y, Levin AV, Enzenauer RW, Elder JE, Letourneau MA, Humphreys RP et al. Retinal findings following accidental head trauma in infants and young children. Ophthalmology 1992; 99: 1718–1723.
Bechtel K, Stoessel K, Leventhal JM, Ogle E, Teague B, Lavietes S et al. Characteristics that distinguish accidental from abusive injury in hospitalized young children with head trauma. Pediatrics 2004; 114: 165–168.
Green MA, Lieberman G, Milroy CM, Parsons MA . Ocular and cerebral trauma in non-accidental injury in infancy: underlying mechanisms and implications for paediatric practice. Br J Ophthalmol 1996; 80: 282–287.
Morad Y, Kim YM, Mian M, Huyer D, Capra L, Levin AV . Nonophthalmologists' accuracy in diagnosing retinal hemorrhages in the Shaken Baby syndrome. J Pediatr 2003; 142: 431–434.
Acknowledgements
We gratefully acknowledge the administrative assistance of our Research Assistant, Enza Perruzza.
Author information
Authors and Affiliations
Corresponding author
Additional information
The authors have no proprietary interest in any of the materials used in this study. This study was supported in part by Brandan's Eye Research Fund
Rights and permissions
About this article
Cite this article
Gnanaraj, L., Gilliland, M., Yahya, R. et al. Ocular manifestations of crush head injury in children. Eye 21, 5–10 (2007). https://doi.org/10.1038/sj.eye.6702174
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6702174
Keywords
This article is cited by
-
The eye in child abuse
Child's Nervous System (2022)
-
Retinale Blutungen und venöse Stase — Sturz oder Misshandlung?
Pädiatrie (2018)
-
Retinale Blutungen und venöse Stase bei einem 10 Monate alten Säugling nach Sturz?
Der Ophthalmologe (2016)
-
The eye in child abuse: Key points on retinal hemorrhages and abusive head trauma
Pediatric Radiology (2014)
-
Retinal haemorrhages and related findings in abusive and non-abusive head trauma: a systematic review
Eye (2013)
