
Abstract
Aims To evaluate the functional effect of bilateral implantation of two different multifocal intraocular lenses (IOL) compared with the standard monofocal IOL.
Methods Sixty-nine patients were recruited into a prospective, double-masked, randomised, controlled trial at a single hospital in the United Kingdom. Sixty completed follow-up; 16 implanted with monofocal IOLs, 29 with AMO ’ARRAY’ multifocal IOLs and 15 with Storz ’TRUEVISTA’ bifocal IOLs. Phacoemulsification and IOL implantation was performed to a standardised technique in both eyes within a 2-month period. The main outcome measures were distance and near visual acuity, depth of field and validated assessment of subjective function (TyPE questionnaire).
Results Unaided distance acuity was good, and equivalent across the three groups. Corrected distance acuity was significantly lower in the bifocal group. Patients with multifocal and bifocal IOLs could read smaller absolute print size than those in the monofocal group (P = 0.05), but at a closer reading distance such that mean unaided near acuity was equal in the three groups. Corrected near acuity was significantly higher in the monofocal control group (P < 0.05). Depth of field was increased in multifocal (P = 0.06) and bifocal (P = 0.004) groups. Overall visual satisfaction was equal in the three groups, while near visual satisfaction was higher in the multifocal group than the monofocal (P = 0.04). Spectacle independence was not seen in the monofocal group, but was achieved in 28% of multifocal IOL patients and 33% of bifocal patients (P < 0.001). Adverse symptoms such as glare and haloes were significantly more bothersome with multifocal (not bifocal) IOLs than monofocals (P = 0.01).
Conclusions Multifocal and bifocal IOLs improved unaided near vision performance, with around one in three patients becoming spectacle-independent. The main adverse effect was an increased incidence of subjective glare and haloes in the multifocal IOL group.
Similar content being viewed by others


Introduction
Modern surgical techniques allied to accurate biometry and use of third generation intraocular lens (IOL) power calculation formulae allow a reasonable expectation of good unaided distance vision following cataract surgery.1,2,3 Standard IOLs are monofocal, having a fixed focal distance; at different object distances blur occurs. Typically, the surgeon aims for emmetropia or low myopia, with reading glasses prescribed for near vision.
Various strategies have been suggested to eradicate the need for reading glasses. Monovision (one eye emmetropic and the other myopic) and myopic astigmatism alter the refractive aim using standard monofocal IOLs. A prospective assessment of spectacle independence with patients in whom the refractive aims of monovision were successfully achieved found only 14% managed without glasses.4 Myopic astigmatism inevitably limits distance acuity5,6,7 which many surgeons would find unacceptable. A zoom principle accommodating IOL has been designed (BioComFold, Morcher, Stuttgart, Germany); unfortunately the anterior-posterior movement induced by accommodation is inadequate to produce the desired increase in effective power.8,9 Animal models using a flexible silicone polymeric gel to fill the capsular bag following lens extraction have failed as a result of capsular fibrosis.10 The most promising approach at present involves modification of the IOL optic to create multiple focal distances (multifocal IOL).
Whether multifocal IOLs are superior to monofocal IOLs has proved difficult to determine because of the difficulty in defining visual quality. Studies need to examine both objective data, such as visual acuity and contrast sensitivity and glare; and subjective data, preferably using validated instruments to measure visual satisfaction and function.
We report the results of a trial of bilateral implantation of multifocal IOLs, in which patients were randomised to implantation with one of two sorts of multifocal IOL or a monofocal control IOL; with the same lens type in each eye. Detailed objective assessment of visual function before and after surgery was complemented by use of a validated instrument to assess subjective visual function.
Materials and methods
Patient selection
Ethical approval for the trial was obtained from the local hospital ethics committee prior to commencement.
Patients listed for cataract surgery at a single hospital eye unit (Hillingdon Hospital NHS Trust, Hillingdon, UK) were identified in clinic at the time of listing and considered for inclusion in the study. Inclusion and exclusion criteria are listed in Table 1.
The study was a prospective, randomised, controlled trial. Written consent was obtained for randomisation within the trial. Patients were informed that the IOL type implanted would not be revealed to them until the completion of the trial. The potential advantages and disadvantages of bifocal/multifocal IOL implantation as compared with monofocal IOL implantation were discussed, and the patient given a detailed patient information sheet. No patients had prior knowledge or queries regarding multifocal/bifocal IOL technology.
Patients were randomly allocated to one of the three types of IOL from sealed envelopes opened on the pre-operative ward round on the day of surgery. Data analysis, including identification of IOL type, was performed by one of the authors (ML) once data collection was completed. At the time of analysis the author was not involved in care of trial patients.
Operative technique and intraocular lenses
Pre-operative assessment for cataract surgery involved keratometry (Topcon KR 7000P autokeratorefractometer, Europe BV) and A-scan biometry (Ophthasonic Image 2000, Teknar, St Louis, MO, USA), all performed by one of two specialist ophthalmic nurses (FG, LL). Once the allocated IOL was known, the implanting surgeon calculated the required IOL power using the SRK/T formula.3 The IOL power predicted to result in the post-operative refraction nearest to emmetropia was chosen.11 If the available IOL powers would result in equal error either side of emmetropia, the higher power IOL was selected.
All procedures were performed by the authors (ML, NL or PB) using a standardised technique under peribulbar or topical anaesthetic. Clear corneal phacoemulsification was performed through a 2.8-mm, self-sealing incision. The incision was placed temporally, or along the steepest corneal meridian if there was ⩾1 dioptre of corneal astigmatism. This was to ensure that the post-operative corneal astigmatism was ⩽1.5 dioptres.12 A continuous circular capsulorrhexis was created. Following phacoemulsification of the nucleus and aspiration of the soft lens matter, the posterior capsule was polished. The anterior capsule rim was not polished. The incision was enlarged to 3.0 mm for the injectable IOLs and 5.5 mm for the rigid bifocal IOL. The IOL was placed within the capsular bag. Sutures were used following insertion of the rigid IOL, and otherwise if clinically indicated. Operative details and any complications were recorded.
Three types of IOLs were used, detailed in Table 2. The Phacoflex (’monofocal’) and Array (’multifocal’) IOLs are of identical materials and design, except for the five concentric rings of progressively varying refractive power to give a maximum near addition of 3.5 D (average 2.8 in spectacle plane) on the anterior surface of the Multifocal Array.13 The TrueVista (’bifocal’) lens is a one-piece rigid lens with three concentric rings in the optic, the middle one of which has a 4 D near addition (average 3.2 D in the spectacle plane).14 Both the multifocal and the bifocal IOLs have a predominantly distance optical zone centrally and are designed to be distance dominant.
Evaluation
Objective assessment
Patient flow is illustrated in Figure 1. The hospital optometrist and the ophthalmic nurse specialist carrying out these tests (LL) were masked as to the nature of the IOL implanted.

Patient flow through the study.
-
1
Distance Visual Acuity (VA). This was measured using Early Treatment for Diabetic Retinopathy Study acuity charts15 (Precision Vision, IL, USA). VA is expressed as the logarithm of the minimum angle of resolution (logMAR) so that a score of 0 equals 6/6. Doubling the visual angle adds 0.3 to the score, so that 6/12 Snellen equals logMAR 0.3. Scoring was by the single-letter method, with O–C confusion ignored.16 Best-corrected and unaided acuity was measured binocularly at distances from 4 m to 1 m as required, generating a range of logMAR scores from −0.3 to 1.68 (equivalent to 6/3 to 6/240 Snellen). If no letters could be read at 1 m then vision was assessed using a ranked scale of Hand Movements, Counting Fingers and Perception of Light and awarded logMAR scores of 1.9, 2.2, 2.5 respectively.17
-
2
Near Visual Acuity (NVA). This was measured using Bailey–Lovie logMAR word reading acuity charts18 (UC Berkeley, CA, USA). Corrected and unaided NVA was measured binocularly. The smallest print size line of which half or more of the words could be correctly identified was recorded. The logMAR acuity was calculated corrected for the patient’s preferred reading distance.
-
3
Depth of Focus. This was measured binocularly. LogMAR acuity was measured with from +3 to −5 dioptres of defocus from the distance prescription placed in a trial frame. Distance acuity through minus defocus requires pseudoaccommodation.
-
4
Contrast Sensitivity (CS). This was measured binocularly under standardised illumination using a Pelli–Robson Contrast Sensitivity Chart (Clement Clarke, UK), at a distance of 1 m as recommended by the manufacturer.19 Single letter scoring was used.20
-
5
Glare Disability (GD). This was assessed using the Brightness Acuity Tester (BAT)21 (Marco, Florida, USA). VA was measured in the right and left eyes without and with the BAT at its brightest setting (400 ft. Lamberts, equivalent to bright sunlight on a white sand beach).22 Glare was calculated as the difference between the two scores.
Subjective assessment
TyPE instrument
This is a questionnaire designed specifically to assess visual disability caused by cataract, with particular emphasis on the need for spectacle correction. It has been validated for use in the United States as a telephone-administered questionnaire23 and in the UK for self-administered use.24 The questions were filled in by the patient, assisted by family or nursing staff as required, between the pre-operative assessment and surgery (pre-op) and just before the post-operative assessment (post-op).
There are questions relating to global measures of vision, and frequency of spectacle wear. Vision-related functional status is assessed in questions on distance and near vision tasks and glare disability.
Long-term follow-up and unmasking
Patients were invited to attend for examination after a mean of 50 weeks after surgery. Unaided near vision was measured and an abbreviated TyPE questionnaire administered. The patients were then informed of their IOL status. The mechanism of the IOL was explained, and a standardised information sheet given to the patient (’training’). This included suggestions on how best to use the IOL for near vision (Figure 2).

Information sheet given to patients with multifocal or bifocal IOLs as part of training for unaided near vision.
Patients were invited to re-attend after a mean of 65 weeks after surgery to allow measurement of any improvement resulting from unmasking and training.
Statistical analysis and power calculation
Multifocal and bifocal IOL results were compared separately against the monofocal IOL control group. Analysis was performed on a ’treatment as administered’ basis (because of the reasons for exclusion, data were not available on most patients excluded post-randomisation). Continuous data were analysed using Student’s t-test. Tests of proportions used the Chi-squared test. Results from the TyPE questionnaire did not fit the normal distribution and were therefore analysed using non-parametric tests. The Kruskal–Wallis test was used to examine the equality of populations between the three groups, and the two-sample Wilcoxon rank-sum (Mann–Whitney) test was used to compare multifocal and bifocal groups individually against the monofocal control group where the Kruskal–Wallis test gave a probability of less than 0.05.
Using data from Javitt23 and Steinert,25 to achieve 80% power at a 5% significance level, 21 patients per group would be required to detect a difference in both primary outcome measures: unaided NVA and subjective near visual function with the TyPE questionnaire.
Results
Sixty-nine patients entered the trial, with nine withdrawals as detailed in Figure 1. Data presented are from the remaining 60 patients (16 monofocal, 29 multifocal and 15 bifocal). Data were available on all 60 patients at 12 weeks following second eye surgery, on 54 patients at a mean of 50 weeks (range 16–88 weeks) and on 41 patients at a mean of 65 weeks (range 34–140 weeks). Demographic and pre-operative visual data are given in Table 3.
There were no major pre-operative surgical complications. There were two cases of iris prolapse pre-operatively (none post-op), two bent haptics (one monofocal, one multifocal) and two split IOLs on insertion (both multifocal). The torn IOLs were brought into the anterior chamber under viscoelastic protection and divided using capsular scissors to allow removal through an unenlarged section. They were each replaced with multifocal IOLs without further complication. ’In-the-bag’ fixation was achieved in all cases. One monofocal wound, two multifocal and all bifocal wounds required suturing. One eye (multifocal IOL) had residual posterior capsular opacity requiring neodymium-ytrium aluminium garnet laser capsulotomy. This was performed prior to post-operative assessment. All other capsules remained clinically clear throughout the study.
Objective results
Refractive outcomes
The refractive outcomes of surgery are presented in Table 4 (average of two eyes). Ninety-three per cent, 88% and 83% of monofocal, multifocal and bifocal eyes respectively were within 1 dioptre of emmetropia (Figure 3).

Cumulative % of patients achieving stated refractive aim. This analysis assumes a prediction of post-operative emmetropia, the actual IOL chosen was that predicting the closest available outcome to emmetropia. There was no difference between groups.
Visual acuity
VA results are summarised in Table 5. Unaided binocular VA was similar in the three groups, with mean logMAR scores of 0.03, 0.06 and 0.10 for monofocal, multifocal and bifocal IOLs. Mean best-corrected binocular VA was −0.01, 0.01 and 0.09 for monofocal, multifocal and bifocal groups. Best-corrected VA was significantly lower in the bifocal group (P = 0.03).
Near vision (reading) is given as logMAR near acuity (NVA) and absolute print size read. 0.3 logMAR is equivalent to 6/12 Snellen and print size N5.3 read at 33 cm. Post-operative pupil size was measured while reading and did not differ between IOL groups (3.1 mm (SD 0.5) monofocal, 3.4 mm (0.7) multifocal, 3.1 mm (0.8) bifocal).
There was no difference in mean binocular unaided NVA between the three groups, at 0.46 (SD 0.16), 0.43 (0.16) and 0.46 (0.21) logMAR for monofocal, multifocal and bifocal groups respectively. NVA improved slightly in all three groups with long-term follow-up, with no further benefit from unmasking and training observed (Figure 4).

Long-term follow-up and effect of unmasking and training. Only data from those patients who attended all three follow-up visits are included (41/60, 68%). There is a small improvement in mean near acuity with time, but no additional effect of training. The first post-op visit was a median of 12 weeks post-op, the second 44 weeks and the 3rd 60 weeks post-op.
Best-corrected NVA was slightly better in the monofocal group (0.22 (0.14)) than in the multifocal (0.30 (0.16)) and bifocal groups (0.39 (0.19), P < 0.05).
Patients with multifocal and bifocal IOLs were able to read smaller print without glasses than those with the monofocal IOL. N5 size print could be read unaided by 2/16 (13%), 9/29 (31%) and 7/15 (47%) of monofocal, multifocal and bifocal patients respectively. The preferred reading distance decreased as the size of the nominal add of the IOL increased, from 42.1 cm for the monofocal (no add), to 32.5 cm for the multifocal (3.5 D add) and 27.8 cm for the bifocal (4 D add). The mean reading spectacle add required was 2.25 D for the monofocal, 1.85 D for the multifocal and 1.39 D for the bifocal.
Depth of focus
The results of defocus testing for the three IOL types are shown in Figure 5. The monofocal plot was symmetrical, with acuity falling away either side of zero defocus. The multifocal and bifocal IOLs retain acuity better as minus defocus is applied. The bifocal lens produced a second peak of acuity at −3 D defocus.

Depth of focus of IOLs. Binocular distance acuity was measured with a 9 dioptre range of defocus from the distance prescription. Retention of acuity with minus defocus indicates pseudoaccommodation with the multifocal and bifocal IOLs.
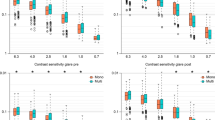
Contrast sensitivity and glare
Mean binocular contrast sensitivity was 1.74 (SD 0.15) for the monofocal IOL, 1.67 (0.13) for the multifocal and 1.65 (0.20) for the bifocal. Glare from the Brightness Acuity Tester had little effect on acuity (LogMAR acuity dropped by 0.02 units with the monofocal IOL, 0.01 units with the multifocal IOL and 0.04 units with the bifocal IOL).
Subjective results: TyPE questionnaire
The parameters relevant to binocular vision addressed by the TyPE questionnaire include visual satisfaction, degree of difficulty with vision-related activities, experience of adverse visual phenomena (Table 6) and use of spectacles (Figure 6). Subjective outcome scores did not fit the normal distribution and are therefore presented as median (range). All scores relate to binocular unaided vision.

Spectacle-independence at last follow-up. 0% of monofocal patients, 28% of multifocals and 33% of bifocals achieved complete independence from spectacle-wear (χ2 = 0.02 and P = 0.005, respectively).
Overall visual satisfaction was 8/10 for all IOLs, while near visual satisfaction was 5/10 (2–8) for the monofocal, 6/10 (0–10) for the multifocal and 7/10 (2–10) for the bifocal (P = 0.20). Difficulty with a range of distance, near and glare-related tasks was scored from 0 (’not at all limited’) to 4 (’extremely limited’). Near vision task difficulty was scored as 1.7 (0–3.4) by the monofocal group, 1.0 (0–3.8) by the multifocal and 0.6 (0–3.4) by the bifocal group (P = 0.22). The TyPE questionnaire also asks the specific question ’Without glasses, how much are you bothered by seeing glare, halo, or rings around light?’, scored from 0 (’not at all bothered’) to 4 (’extremely bothered’). Monofocal and bifocal scores were 0 (0–2) and 0 (0–3) respectively, the multifocal group scored slightly worse, with 1 (0–4) equating to a median score of ’a little bit bothered’ (P = 0.01).
Spectacle independence
Complete freedom from glasses was reported by none of the 16 monofocal patients, seven of the 29 multifocal patients (24%) and one of the 15 bifocal patients (7%) in the 12-week period following their second eye surgery. By the time of the follow-up examination (50 weeks post-op) 0/16, 8/29 (28%) and 4/15 (27%) of monofocal, multifocal and bifocal patients respectively were spectacle-independent. One further bifocal patient did not require spectacles when re-assessed following unmasking and training, making a total of 5/15 (33%) spectacle-independent.
Discussion
Validity
The three groups of patients reported in this study are unbalanced with respect to number of patients, a weakness of an unblocked envelope method of randomisation with the allocation code not being broken until recruitment was complete. Because of the relatively small numbers assigned to the monofocal and bifocal groups, study power for the primary outcome measure of unaided near acuity was slightly lower than planned at 78%. Allocation concealment was carefully maintained, and the authors do not consider that this imbalance indicates bias.
Although the differences were not statistically significant, there were more men and more patients who were drivers prior to surgery in the monofocal IOL group. There is no reason to suggest that the proportion of men would affect outcomes. A high proportion of drivers in a group would not affect the primary outcome of near visual function, but might lead to reduced satisfaction if problems of poor distance acuity or excess glare arose.
Post-operative refractive errors were small, with the percentage of cases within 0.5 and 1 D of intended as good as published standards of accuracy of refractive outcome prediction.26 This is important in that it enables spectacle-dependence and unaided distance and near acuity to be measured without the confounding variable of refractive error.
Visual acuity
Unaided and corrected distance VA was good with all three IOLs. The small reduction in best-corrected acuity in the bifocal group when compared with the control group is unlikely to be clinically significant.
Near vision is harder to assess because of the lack of standardisation of measurement. Near vision is often described with reference to print size, which has the advantage of being easily related to functional reading ability. Alternatively, near acuity (NVA) may be measured, which is dependent on both the print size and reading distance. NVA might be high because of near focusing ability (IOL multifocality) or high ocular resolution in association with blur tolerance. Mean logMAR near acuity was not increased by use of the multifocal or bifocal IOLs in this study (Table 5). The mean acuity was consistent across the three groups at 0.46, 0.43 and 0.46 logMAR for monofocal, multifocal and bifocal IOLs respectively. This value is similar to that achieved by the monofocal control groups in other studies.25,27,28
Patients with multifocal and bifocal IOLs were however more likely to be able to read small print unaided than were those with monofocal IOLs: 13%, 31% and 47% of monofocal, multifocal and bifocal patients respectively were able to read N5 print (P = 0.03). This did not result in increased acuity because the corresponding reading distances also reduced, in proportion to the size of the IOL reading add (Table 5). The only other published randomised trial of bilateral multifocal vs monofocal IOL implantation27 reports unaided logMAR near acuity of 0.11 (Array multifocal) and 0.30 (monofocal) with a total of 232 patients. There is no apparent reason for this difference, as both studies used logMAR reading charts, with acuity calculated corrected for reading distance.
In contrast to the lack of improvement in mean near acuity, examination of the depth of focus plots (Figure 5) illustrates that the multifocal and bifocal IOL patients were able to use their IOLs to accommodate to overcome the effect of minus lens defocus. The defocus curves fit well with those predicted from the optical design of the IOLs.13,14,29 The visual environment in which depth of field is tested, using trial frames and a distance acuity chart, may help explain why defocus-simulated near acuity was better than measured reading acuity. For the depth of field test the patient is limited to one visual target in a defined position, reducing visual confusion due to simultaneous vision.
Subjective outcomes
Visual satisfaction and functionality was similar in the three groups (Table 6), although there was a trend towards improved near visual satisfaction and near vision task difficulty with the multifocal and bifocal IOLs that would probably become statistically significant with more numbers.
Multifocal IOL patients reported significantly more bother from glare/haloes; lack of associated glare-task difficulty, retention of visual acuity with glare, and conversations with patients suggest that the main problem is haloes around light sources rather than glare. Haloes are the blur circles from near and intermediate focus portions of the optic and as such are an inevitable consequence of the design of the multifocal IOL. The size of the halo can be reduced by aiming for low hypermetropia with IOL selection, so that the near focus is closer to the retina and its blur circle smaller. In this study we elected to aim for emmetropia so as not to compromise unaided distance acuity or reduce the likelihood of achieving unaided reading vision. The bifocal IOL was reported as causing less bother from haloes, which may reflect its simpler design, with only two, rather than multiple, focal points.
Spectacle-independence was achieved by at least 28% and 33% of multifocal and bifocal IOL patients respectively at approximately a year following surgery. This is similar to other trials using the TyPE to assess spectacle usage (41%,23 32%27), and was not seen with monofocal IOL implantation. Reported success rates with refractive multiple focus contact lenses are higher than with multifocal IOLs (58%,30 53%,31 58.7%32), presumably because of the ability to adjust distance power and near addition and the younger age of contact lens wearers relative to cataract patients. A 50% rate of spectacle-independence is probably a realistic maximum expectation for the multifocal IOL. Of course, reduced dependence on spectacles short of total independence may still provide a worthwhile benefit to patients.
It is likely that the failure of a proportion of multifocal IOL patients to achieve functional multifocality results from a failure to select the correct image in a situation of simultaneous vision. In other words, the process of image selection is not intuitive or spontaneous in all patients. The authors are not aware of any published work on the effect of training in the use of these IOLs. We observed an improvement in near acuity with time in all three IOL groups and an increase in spectacle-independence in multifocal and bifocal patients, but no evidence for further benefit accruing from training in multifocal or bifocal IOL use.
Conclusions
The multiple focus optic IOL is a useful addition to the tools available to the cataract surgeon. The bifocal and the multifocal IOLs examined performed similarly although there was a higher incidence of bothersome haloes with the multifocal IOL. The ease of use and reliable astigmatic neutrality of the injectable ’Array’ is however an advantage over the rigid PMMA ’TrueVista’.
Improved depth of focus and near visual function is achieved with these IOLs when compared with the monofocal standard, but only a minority will achieve complete freedom from spectacles. Patient satisfaction is likely to be highest if the multifocal IOLs are reserved for patients who express a desire for spectacle-independence but who are realistic about the likelihood of achieving this aim.
References
Desai P, Reidy A, Minassian D . The National Cataract Surgery Survey 1997/98. A report of the results of the clinical outcomes. Br J Ophthalmol 1999; 83: 1336–1340
Desai P, Reidy A, Minassian D, Vafidis G, Bolger J . Gains from cataract surgery: visual function and quality of life. Br J Ophthalmol 1996; 80: 868–873
Retzlaff J, Sanders D, Kraff M . Development of the SRK/T intraocular lens implant power calculation formula. J Cataract Refract Surg 1990; 16: 333–340
Boerner C, Thrasher B . Results of monovision correction in bilateral pseudophakes. Am Intra-ocular Implant Soc J 1984; 10: 49–51
Sawsuch M, Guyton D . Optimal astigmatism to enhance depth of focus after cataract surgery. Ophthalmology 1991; 98: 1025–1029
Hillman J, Bradbury . Apparent accommodation by myopic astigmatism with monofocal intraocular lenses. Eur J Implant Ref Surg 1990; 2: 101–104
Datiles M, Gancayco T . Low myopia with low astigmatic correction gives cataract surgery patients good depth of focus. Ophthalmology 1990; 97: 922–926
Legeais J-M, Werner L, Werner L, Abenheim A, Renard G . Pseudoaccommodation: BioComFold versus a foldable silicone intraocular lens. J Cataract Refract Surg 1999; 25: 262–267
Leyland M, Bloom P . Intraocular lens design for pseudoaccommodation (letter). J Cataract Refract Surg 1999; 25: 1038–1039
Haefliger E, Parel J . Accommodation of an endocapsular silicone lens (Phaco-Ersatz) in the aging rhesus monkey. J Refract Corneal Surg 1994; 10: 550–555
Holladay J, Hoffer K . Intraocular lens power calculations for multifocal intraocular lenses. Am J Ophthalmol 1992; 114: 405–408
Kershner R . Clear corneal cataract surgery and the correction of myopia, hyperopia, and astigmatism. Ophthalmology 1997; 104: 381–389
Fine I . Design and early clinical studies of the AMO Array multifocal IOL. In: Maxwell WA, Nordan LT (eds). Current Concepts of Multifocal Intraocular Lenses Slack: Thorofare, NJ 1991 105–115
Neubert W, Hsia T, Green G, Jones M, McCary B, Kastigar S, Bedoya J . Technical Monograph of the TRUEVISTA Multifocal Intraocular Lens Storz: St Louis, USA
Ferris F, Kassof A, Bresnick G, Bailey I . New visual acuity charts for clinical research. Am J Ophthalmol 1982; 94: 91–96
Bailey I, Lovie J . New design principles for visual acuity letter charts. Am J Optom Physiol Opt 1976; 53: 740–745
Javitt J, Brenner H, Curbow B, Legro M, Street D . Outcomes of cataract surgery. Improvement in visual function after surgery in the first, second and both eyes. Arch Ophthalmol 1993; 111: 686–691
Bailey I, Lovie J . The design and use of a new near vision chart. Am J Optom Physiol Opt 1980; 57: 378–387
Pelli D, Robson J, Wilkins A . The design of a new letter chart for measuring contrast sensitivity. Clin Vision Sci 1998; 2: 187–199
Elliott D, Bullimore M, Bailie I . Improving the reliability of the Pelli-Robson contrast sensitivity test. Clin Vis Sci 1991; 6: 471–475
Holladay J, Prager T, Trujillo J, Ruiz R . Brightness acuity test and outdoor visual acuity in cataract patients. J Cataract Refract Surg 1987; 13: 67–69
Prager T, Urso R, Holladay J, Stewart R . Glare testing in cataract patients: instrument evaluation and identification of sources of methodological error. J Cataract Refract Surg 1989; 15: 149–157
Javitt J, Wang F, Trentacost D, Rowe M, Tarantino N . Outcomes of cataract extraction with multifocal intraocular lens implantation: functional status and quality of life. Ophthalmology 1997; 104: 589–599
Lawrence D, Brogan C, Benjamin L, Pickard D, Stewart-Brown S . Measuring the effectiveness of cataract surgery: the reliability and validity of a visual function outcomes instrument. Br J Ophthalmol 1999; 83: 66–70
Steinert R, Aker B, Trentacost D, Smith P, Tarantino N . A prospective comparative study of the AMO ARRAY zonal-progressive multifocal intraocular lens and a monofocal intraocular lens. Ophthalmology 1999; 106: 1243–1255
Olsen T, Bargum R . Outcome monitoring in cataract surgery. Acta Ophthalmol Scand 1995; 73: 433–437
Javitt J, Steinert R . Cataract extraction with multifocal intraocular lens implantation. A multinational clinical trial evaluating clinical, functional, and quality-of-life outcomes. Ophthalmology 2000; 107: 2040–2048
Steinert R, Post C, Brint S, Fritch C, Hall D, Wilder L et al. A prospective, randomized, double-masked comparison of a zonal-progressive multifocal intraocular lens and a monofocal intraocular lens. Ophthalmology 1992; 99: 853–861
Holladay J, van Dijk H, Lang A, Portney V, Willis T, Sun R, Oksman H . Optical performance of multifocal intraocular lenses. J Cataract Refract Surg 1990; 16: 413–422
Sheedy J, Harris M, Bronge M, Joe S, Mook M . Task and visual performance with concentric bifocal contact lenses. Optom Vis Sci 1991; 68: 537–541
Key J, Morris K, Mobley C . Prospective evaluation of Sunsoft multifocal contact lens. CLAO J 1996; 22: 179–184
Key J, Yee J . Prospective evaluation of the Acuvue bifocal contact lens. CLAO J 1999; 25: 218–221
Acknowledgements
Presented in part at the American Acadamy of Ophthalmology, Dallas, 23 October 2000 and at the Royal College of Ophthalmologists Annual Congress, Birmingham 22–24 May 2001.
The authors have no financial interest in any of the products described in this paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Leyland, M., Langan, L., Goolfee, F. et al. Prospective randomised double-masked trial of bilateral multifocal, bifocal or monofocal intraocular lenses. Eye 16, 481–490 (2002). https://doi.org/10.1038/sj.eye.6700077
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.eye.6700077
Keywords
This article is cited by
-
Multifocal intraocular lenses and retinal diseases
Graefe's Archive for Clinical and Experimental Ophthalmology (2020)
-
Effectiveness of multifocal and monofocal intraocular lenses for cataract surgery and lens replacement: a systematic review and meta-analysis
Graefe's Archive for Clinical and Experimental Ophthalmology (2019)
-
State of the art of intraocular lens manufacturing
The International Journal of Advanced Manufacturing Technology (2018)
-
Monovision Versus Multifocality for Presbyopia: Systematic Review and Meta-Analysis of Randomized Controlled Trials
Advances in Therapy (2017)
-
A Comparison of a Monofocal Acrysoft IOL Using the “Blended Monovision” Formula with the Multifocal Array IOL for Glasses Independence After Cataract Surgery
Annals of Ophthalmology (2007)
