
Abstract
In one geographical area, 14 high-risk human papillomavirus types in cervical intraepithelial neoplasia (CIN2/3; n=139) and cervical squamous cell carcinoma (SCC; n=84) were analysed. HPV18 was more prevalent in SCC than CIN2/3 (OR 9.8; 95% confidence interval: 2.5–39). Other high-risk types prevalences corresponded in CIN2/3 and SCC. Evaluations using CIN2/3 as a measure of efficiency underestimate the contribution of HPV18 to SCC.
Similar content being viewed by others


Main
Human papillomavirus (HPV) infections are the cause of cervical cancer and its precursors lesions (Walboomers et al, 1999). So far, 15 HPV types have been classified as high-risk types, and three types have been classified as probable high risk (Munoz et al, 2003). Within the group of high-risk HPV (hrHPV) types, different types seem to confer different degrees of risk for cervical cancer and its precursor lesions (Clifford et al, 2006). A markedly increased risk of cervical cancer has been attributed to HPV16 and HPV18, as prevalence studies have shown that 60–70% of cervical squamous cell carcinoma (SCC) cases are positive for HPV16 or HPV18 (Munoz et al, 2003).
As a consequence, assessment of the additive value of HPV typing in cervical screening is the subject of many ongoing studies. However, screening evaluations generally use high-grade cervical intraepithelial neoplasia (CIN2/3) as intermediate end point of cervical cancer. This may lead to underestimation or overestimation of the contribution of certain HPV types in case the HPV type distribution between CIN2/3 and cervical cancer differs. Indeed, several studies suggest that HPV18 is underrepresented in CIN2/3 compared to SCC (Bulkmans et al, 2005; Castle et al, 2005; Khan et al, 2005), and in a meta-analysis as well (Clifford et al, 2006).
Here, we address type distribution of different hrHPV types in CIN2/3 and SCC samples collected in one geographical area.
Materials and methods
Study selection
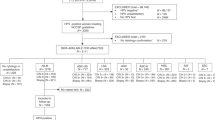
From the archives of the Department of pathology of Ziekenhuis Walcheren in The Netherlands, we identified 187 specimens of CIN2/3 (87 CIN2 and 100 CIN3) diagnosed after screening between 1996 and 2000, and 90 specimens of SCC from the period 1981 to 1998. The department of pathology serves the population of the Walcheren peninsula, where follow-up of screened women is approximately 90% complete. All histological samples were collected retrospectively and were subjected to revision. The Medical Ethics Committee of VU University Medical Center approved the study (2001/179).
HPV testing
Representative samples of the formalin-fixed biopsies were processed for PCR analysis (Walboomers et al, 1999; Jacobs et al, 2000). Amplification of a 209 base-pair fragment of the β-globin gene was performed to test the integrity of DNA (Roda Husman et al, 1994). Detection of hrHPV was performed by GP 5+/6+ consensus primer PCR enzyme immunoassay, using a cocktail of 21 low-risk types and 14 high-risk types. All HPV-positive samples were typed by reverse line blotting (van den Brule et al, 2002). We tested for hrHPV16, 18, 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68 and lrHPV6, 11, 32, 40, 42, 43, 44, 54, 55, 57, 61, 70, 71, 72, 81, 83, 84, 85, 86, cp6108 and jc9710 (Jacobs et al, 1997). In addition, all GP5+/6+ PCR-negative samples were evaluated by E7 region type-specific PCR for the same 14 high-risk types to exclude the presence of hrHPV in integrated form and/or loss of the GP5+/6+ primer-binding region (Walboomers et al, 1999). Technicians performing PCR analysis were blinded for histological classification of samples.
Study material
Formalin-fixed archival material could not be retrieved for 17 cases with CIN2/3. Of the women with CIN2/3, 21 samples tested HPV-negative and in seven cases, only low-risk types could be identified. One case tested hrHPV-positive without identifying a specific high-risk type, leaving 139 cases of CIN2/3 with known hrHPV type for statistical analysis. Of the women with SCC, seven cases tested negative for HPV by both assays, leaving 83 cases with SCC and a known hrHPV type for statistical analysis.
Statistical analysis
Differences in prevalence of hrHPV types for CIN2/3 compared to SCC were examined using the Mantel-Haenszel common odds ratio (ORMH) and 95% confidence intervals (95% CIs). Statistical significance was tested by Cochran's Mantel-Haenszel test. Data were stratified by age (i.e., below 29 years, 29–33, 34–38, 39–43, 44–48, 49–53, 54–58, 59–61 and 62 years and over) and whether infections were single or multiple. The presence of an association between ORMH and age was tested by Breslow–Day's test of homogeneity. Analyses were repeated for women with single infections only.
The presented results may not be free of hidden bias as there is some evidence that HPV18-positive lesions are underrated by cytology (Woodman et al, 2003; Berkhof et al, 2006). Therefore, it cannot be excluded that prevalence differences of certain hrHPV types in CIN2/3 compared to SCC is associated with cytological screening failures. We examined the influence of hidden bias by computing an adjusted P-value obtained under the assumption that among the hrHPV-positive CIN2/3 and SCC cases, the odds of observing a certain hrHPV type in SCC compared to CIN2/3 differed by a factor 2 (Rosenbaum (1991).
Results
The mean age of women with CIN2/3 (n=139) was 37 years (range 26–57 years). Women with SCC (n=84) had a mean age of 49 years (range 27–88 years). The mean age of women with SCC was higher than the mean age of women with CIN2/3 (P<0.001). Multiple HPV infections were present in 9.4% (13 out of 139) of CIN2/3, and in 10.8% (9 out of 83) of SCC (P=0.719).
Table 1 displays the hrHPV type-specific prevalence rates in women with CIN2/3 compared to SCC. In women with CIN2/3, 59.7% of hrHPV positivity was due to HPV16 and 12.9% to HPV31. Another 2.9% of hrHPV infections were HPV18 and 11.5% HPV52 positive. In women with SCC, 69.9% of hrHPV positivity was due to HPV16. HPV31 was present in 7.2% of cases, and HPV18 in 12.0%. No SCC cases tested positive for HPV52 in this study. Type-specific prevalences did not substantially change when analysing women with single infections separately.
Women having SCC carried HPV16 more often than women with CIN2/3, although the estimated ORMH was not statistically significant (ORMH 1.5; 95% CI: 0.8–3.1). The prevalence of HPV18 was significantly higher in SCC than in CIN2/3 (ORMH 8.3; 95% CI: 1.9–36). The other high-risk HPV types were not associated with increased risks individually, but when all hrHPV-positive infections without HPV16 and HPV18 were analysed as one group, the result was significant (ORMH 0.4; 95% CI: 0.2–0.8). For none of the HPV types OR varied with age (data not shown). Results for single infections were comparable.
Even when assuming that the odds to detect an HPV18-associated SCC compared to an HPV18-associated CIN2/3 differed by a factor 2, HPV18 would still be increased in SCC compared to CIN2/3 (P=0.035).
Discussion
In this cross-sectional study, we compared hrHPV type-specific prevalence in CIN2/3 and invasive carcinomas in women identified through population-based cervical screening in a geographically restricted area. We demonstrated that HPV18 prevalence is increased in SCC compared to premalignant lesions. In addition, this study underlines the previously recognised importance of HPV16 for the development of SCC. Other types did not show a prevalence difference.
The increased prevalence of HPV18 in cervical cancer compared to CIN2/3 as found in our study is in agreement with a recent meta-analysis and data from Australia, South Africa and the US (Clifford et al, 2003; Kay et al, 2003; Zuna et al, 2004). The sample size of our study was slightly low, because CIN2/3 and SCC cases were collected from one restricted geographical area. Nonetheless, we were able to demonstrate effects of HPV18 in SCC. Our study cannot differentiate between increased progression risks of HPV18 for the transition of CIN2/3 to SCC as an explanation of our findings, and underdetection of screen-diagnosed CIN2/3 lesions associated with HPV18 as an alternative theory. Our previous, cross-sectional study indicated a preferential risk of HPV18 for the development of cancer from normal cytology (Bulk et al, 2006). However, the estimate of the risk associated with HPV18 for cervical cancer compared to CIN2/3 obtained in this study is rather high (ORMH 9.7; 95% CI: 2.4–39). To calculate approximately how robust this finding is against underdetection of HPV18-associated lesions by cytology in a cervical screening programme (Woodman et al, 2003), we estimated the prevalence difference of HPV18 between CIN2/3 and SCC using a sensitivity analysis. We found that the difference in HPV18 prevalence between CIN2/3 and SCC still remains statistically significant, even if the detection of HPV18-associated CIN2/3 lesions through screening compared to HPV18-positive SCC cases is underestimated by a factor 2. Underrepresentation of HPV18-associated lesions might be explained by the finding that HPV18 infections often occur high in the endocervical canal where lesions are less accessible to screening. Nevertheless, whether the observed association between HPV18 and SCC is mainly caused by a preferential risk of HPV18 for the development if SCC, or by underdetection of HPV18 precursor lesions, our findings have important implications for evaluations of screening programmes. Currently, most, if not all, screening programmes use CIN2/3 as an intermediate end point for cervical cancer to evaluate screening efficacy. This approach seriously underestimates the contribution of HPV18 to the development of SCC. As a consequence, vaccination to HPV16 and HPV18 will decrease HPV18-associated carcinoma incidence more than short-term studies using CIN2/3 as an outcome measure indicate.
In conclusion, HPV18 prevalence is high in invasive SCC compared to CIN2/3 lesions. Thus, when CIN2/3 is used as intermediate end point for cervical cancer, the contribution of HPV18 to the development of invasive SCC is underestimated. As the vast majority of both SCC and adenocarcinomas is attributable to HPV16 and HPV18, women with screen-detected HPV16 and HPV18 infections should be offered more intensive follow-up schemes compared to women infected with other high-risk HPV types.
Change history
16 November 2011
This paper was modified 12 months after initial publication to switch to Creative Commons licence terms, as noted at publication
References
Berkhof J, Bulkmans NW, Bleeker MCG, Bulk S, Snijders PJF, Voorhorst FJ, Meijer CJLM (2006) HPV type-specific 18-month risk of high-grade cervical intraepithelial neoplasia in women with a normal or borderline/mildly dyskaryotic smear. Cancer Epidemiol Biomarkers Prev 15: 1268–1273
Bulk S, Berkhof J, Bulkmans NW, Zielinski GD, Rozendaal L, van Kemenade FJ, Snijders PJ, Meijer CJ (2006) Preferential risk of HPV16 for squamous cell carcinoma and of HPV18 for adenocarcinoma of the cervix compared to women with normal cytology in The Netherlands. Br J Cancer 94: 171–175
Bulkmans NW, Bleeker MC, Berkhof J, Voorhorst FJ, Snijders PJ, Meijer CJ (2005) Prevalence of types 16 and 33 is increased in high-risk human papillomavirus positive women with cervical intraepithelial neoplasia grade 2 or worse. Int J Cancer 117: 177–181
Castle PE, Solomon D, Schiffman M, Wheeler CM (2005) Human papillomavirus type 16 infections and 2-year absolute risk of cervical precancer in women with equivocal or mild cytologic abnormalities. J Natl Cancer Inst 97: 1066–1071
Clifford G, Franceschi S, Diaz M, Munoz N, Villa LL (2006) Chapter 3: HPV type-distribution in women with and without cervical neoplastic diseases. Vaccine 24 Suppl 3: S26–S34
Clifford GM, Smith JS, Aguado T, Franceschi S (2003) Comparison of HPV type distribution in high-grade cervical lesions and cervical cancer: a meta-analysis. Br J Cancer 89: 101–105
Jacobs MV, Snijders PJ, van den Brule AJ, Helmerhorst TJ, Meijer CJ, Walboomers JM (1997) A general primer GP5+/GP6(+)-mediated PCR-enzyme immunoassay method for rapid detection of 14 high-risk and 6 low-risk human papillomavirus genotypes in cervical scrapings. J Clin Microbiol 35: 791–795
Jacobs MV, Zielinski D, Meijer CJ, Pol RP, Voorhorst FJ, de Schipper FA, Runsink AP, Snijders PJ, Walboomers JM (2000) A simplified and reliable HPV testing of archival Papanicolaou-stained cervical smears: application to cervical smears from cancer patients starting with cytologically normal smears. Br J Cancer 82: 1421–1426
Kay P, Soeters R, Nevin J, Denny L, Dehaeck CM, Williamson AL (2003) High prevalence of HPV 16 in South African women with cancer of the cervix and cervical intraepithelial neoplasia. J Med Virol 71: 265–273
Khan MJ, Castle PE, Lorincz AT, Wacholder S, Sherman M, Scott DR, Rush BB, Glass AG, Schiffman M (2005) The elevated 10-year risk of cervical precancer and cancer in women with human papillomavirus (HPV) type 16 or 18 and the possible utility of type-specific HPV testing in clinical practice. J Natl Cancer Inst 97: 1072–1079
Munoz N, Bosch FX, de Sanjose S, Herrero R, Castellsague X, Shah KV, Snijders PJ, Meijer CJ (2003) Epidemiologic classification of human papillomavirus types associated with cervical cancer. N Engl J Med 348: 518–527
Roda Husman AM, Walboomers JM, Meijer CJ, Risse EK, Schipper ME, Helmerhorst TM, Bleker OP, Delius H, van den Brule AJ, Snijders PJ (1994) Analysis of cytomorphologically abnormal cervical scrapes for the presence of 27 mucosotropic human papillomavirus genotypes, using polymerase chain reaction. Int J Cancer 56: 802–806
Rosenbaum PR (1991) Discussing hidden bias in observational studies. Ann Intern Med 115: 901–905
van den Brule AJ, Pol R, Fransen-Daalmeijer N, Schouls LM, Meijer CJ, Snijders PJ (2002) GP5+/6+ PCR followed by reverse line blot analysis enables rapid and high-throughput identification of human papillomavirus genotypes. J Clin Microbiol 40: 779–787
Walboomers JM, Jacobs MV, Manos MM, Bosch FX, Kummer JA, Shah KV, Snijders PJ, Peto J, Meijer CJ, Munoz N (1999) Human papillomavirus is a necessary cause of invasive cervical cancer worldwide. J Pathol 189: 12–19
Woodman CB, Collins S, Rollason TP, Winter H, Bailey A, Yates M, Young LS (2003) Human papillomavirus type 18 and rapidly progressing cervical intraepithelial neoplasia. Lancet 361: 40–43
Zuna RE, Allen RA, Moore WE, Mattu R, Dunn ST (2004) Comparison of human papillomavirus genotypes in high-grade squamous intraepithelial lesions and invasive cervical carcinoma: evidence for differences in biologic potential of precursor lesions. Mod Pathol 17: 1314–1322
Acknowledgements
We thank Dr Elle K.J. Risse for revision of histological specimens and all technicians from the Streeklaboratorium Zeeland (Middelburg, The Netherlands), especially F. Peters, for their help in retrieving the cases from the PALGA and providing all histological samples included in the study. We are indebted to Dr G.D. Zielinski for collecting the carcinoma samples, to M.C.G.T. Verkuijten and R.P. Pol for hrHPV typing and to Dr F.J. Voorhorst for helpful comments on this paper.
This study was supported by grants 28-2831 and 2200.0089 from the Health Research and Development Council of the Netherlands (ZonMw). The study was approved by the Medical Ethics Committee of the VU University Medical Center, Amsterdam, The Netherlands (2001/179)This study was supported by grants 28-2831 and 2200.0089 from the Health Research & Development Council of the Netherlands (ZonMw).S. Bulk performed the analyses and wrote the manuscript. J Berkhof was responsible for the statistical methods. PJF Snijders and CJLM Meijer were responsible for the virology determinations. J Berkhof and CJLM Meijer were responsible for the study design. All investigators discussed findings and critically revised the paper.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
From twelve months after its original publication, this work is licensed under the Creative Commons Attribution-NonCommercial-Share Alike 3.0 Unported License. To view a copy of this license, visit http://creativecommons.org/licenses/by-nc-sa/3.0/
About this article
Cite this article
Bulk, S., Berkhof, J., Rozendaal, L. et al. The contribution of HPV18 to cervical cancer is underestimated using high-grade CIN as a measure of screening efficiency. Br J Cancer 96, 1234–1236 (2007). https://doi.org/10.1038/sj.bjc.6603693
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bjc.6603693
Keywords
This article is cited by
-
Carcinogenesis and management of human papillomavirus-associated cervical cancer
International Journal of Clinical Oncology (2023)
-
Differential expression of human papillomavirus 16-, 18-, 52-, and 58-derived transcripts in cervical intraepithelial neoplasia
Virology Journal (2020)
-
High-resolution genomic profiling of human papillomavirus-associated vulval neoplasia
British Journal of Cancer (2010)
