
Abstract
In routine prenatal diagnostics we used a commercial multiplex ligation-dependent probe amplification (MLPA) kit for aneuploidy screening for chromosomes 13, 18, 21, X and Y. We present the results of 1593 consecutive prenatal samples analysed and diagnosed prior to knowledge of the G-banding analysis during 8-month routine use of computer-assisted MLPA aneuploidy screening. In total, 27 aneuploidies were detected. There were no false positive results while two false negative results could be explained by a placental mosaicism and a partial monosomy, respectively. In total, 3.2% of the samples were inconclusive. We conclude that automatic computer assisted MLPA is a rapid, simple and reliable method for detection of aneuploidies in prenatal diagnostics.
Similar content being viewed by others

Introduction
To reduce the waiting time associated with prenatal chromosome analysis, a number of methods based on uncultured chorionic villi or amniocytes have been developed. The methods aim at screening for the most common aneuploidies, that is, of chromosomes 13, 18, 21, X and Y. The result is available within 24–48 h and followed up by conventional karyotyping on cultured cells. Aneuploidy screening by interphase FISH using commercially available probes has successfully been in routine use for the last 5–10 years, while quantitative fluorescent PCR (QF-PCR) analysis, based on polymorphic small tandem repeats (STR) markers from chromosome 13, 18, 21, X and Y more recently, has been successfully introduced to replace FISH analysis (reviewed in Hultén et al1). Multiplex ligation-dependent probe amplification (MLPA) is yet another recent technique allowing relative quantification of about 40 different DNA sequences in a single reaction.2 A commercially available MLPA aneuploidy screening kit contains 32 specific probes for the chromosomes 13, 18, 21, X and Y (SALSA P001 Trisomy test kit, MRC-Holland, Amsterdam, The Netherlands). We present the results of 1593 consecutive prenatal samples analysed by computer assisted MLPA analysis. While collecting the data, a test of the MLPA aneuploidy kit in a routine setting was published by others.3
Material and methods
Samples
From mid-March to mid-November 2003, 1614 amniotic and chorionic villus samples (CVS) were referred to the Cytogenetic Laboratory for karyotyping and MLPA aneuploidy screening. Eight samples were excluded from MLPA analysis mainly because of too little sample material. In total, 13 samples were excluded from karyotyping; six because of too little sample material and seven because of cultivation failure. Thus, the remaining 1593 samples (809 amniotic samples and 784 CVS) were both karyotyped and analysed by MLPA. Inconclusive MLPA results were mailed; abnormal findings of MLPA and G-banding analysis were reported by telephone while normal results were mailed in two turns. It was the aim that the result of the MLPA analysis should be completed and replied within 2 days from receipt of the sample.
Sample preparation and analysis
DNA from 3–4 ml amniotic fluid or 5 mg chorionic villus samples was isolated using a QIAamp kit (Qiagen, Hilden, Germany), according to the manufacturer's instruction. DNA yield was in the range of 0.3–2.0 μg. In total, 20–100 ng DNA was used in the MLPA aneuploidy protocol according to the manufacturer's instructions. Reactions were performed on a GeneAmp PCR System 9700 (Applied Biosystems, Foster City, CA, USA). A measure of 2 μl PCR product were analysed by capillary electrophoresis on an ABI Prism 3100 Genetic Analyzer (Applied Biosystems) and quantitative data were extracted by ABI Prism GeneScan Analysis software (Applied Biosystems). G-banding analysis was carried out by standard techniques.
Computer-assisted MLPA aneuploidy analysis
Following capillary electrophoresis, each probe peak area is normalised in relation to the neighbouring peak areas of the test sample. The ratio for each peak area is calculated relative to a standard reference created from normal samples. The mean ratio value and SD are calculated for each of the chromosomes 13, 18, 21, X, and Y, and the significance for being outside a reference interval around ratio 1.0 is tested. P⩽1% suggests aneuploidy and 1%<P⩽5% suggests potential aneuploidy. Sample quality is automatically assessed and a diagnosis is suggested.
Details regarding the software for automatic analysis will be published elsewhere; further information is also available by application to the authors.
Results
From mid-March to mid-November 2003, MLPA was offered as a routine analysis at the Department of Clinical Genetics. Results were evaluated on the basis of plots of the ABI capillary electrophoresis and the corresponding data sheet produced by the automatic software. If an MLPA analysis had poor technical quality or a result for some reason was doubted, the MLPA analysis was repeated.
Results of the MLPA analyses were completed and a diagnosis was provided before knowledge of the G-banded karyotypes. The results of both techniques are compared in Table 1.
No incorrect MLPA results were reported. 1542 (96.8%) of the 1593 replies were conclusive whereas 51 (3.2%) were ‘Inconclusive’. The MLPA analysis was repeated in 197 cases (12.4% of 1593).
Table 2 and 3 show the assignments made by fully automatic MLPA analysis of the 1542 prenatal samples that had conclusive replies and the 51 prenatal samples that were replied as ‘Inconclusive’, respectively.
Analysis of the 197 cases that were repeated showed that 146 of the cases were automatically assigned as ‘Poor quality’.
Discussion
MLPA is an attractive technique for aneuploidy screening in a diagnostic routine laboratory. Compared to FISH it allows processing of a large number of samples and in contrast to QF-PCR a commercially kit is available. Additionally, the costs are reasonable (approximately 100 EUR per sample, all included). To our knowledge the present study is the first where computer assisted aneuploidy screening based on the MLPA technique was used in routine prenatal diagnostics. As seen in Table 1, 27 aneuploidies were detected by MLPA and no false positive results were reported among 1593 consecutive samples.
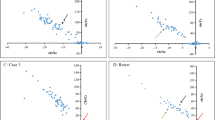
A CVS showing 47,XXX by G-banding analysis was diagnosed by MLPA as 46,XX. However, subsequent MLPA analysis of cultivated cells also revealed trisomy X suggesting that the original discrepancy was caused by different cell lines being analysed by the two techniques. Thus, the 46,XX karyotype probably represented cytotrophoblast cells while the mesodermal core cells carried the 47,XXX karyotype. Similar discordance has been described between direct CVS preparations and villus/foetal cultures.4 Only recently we experienced a CVS showing trisomy 18 in MLPA analysis but normal karyotype in the G-banding analysis of the cultured cells and a follow-up amniotic fluid sample. These examples of cytogenetic inconsistencies demonstrate the need for attentive line of action when an abnormal MLPA result from a CVS sample is not accompanied by abnormal results of ultrasound examination or serum screening.
A case of 69,XXY was assigned as ‘Contamination by maternal DNA’ and was concluded to be ‘Inconclusive’, as the diagnosis ‘69,XXY’ was not added until a later version of the analysis software. Yet, as the MLPA technique is unable to discriminate between a sample contaminated by maternal DNA and a sample carrying a 69,XXY karyotype, the latter diagnosis would only be of significance if it were associated with ultrasound examination indicating triploidy. Besides, interphase FISH analysis is indicated in cases where triploidy is suspected.
MLPA analysis was performed twice in a case showing 46,XX,del(18)(q21 → qter) by G-banding. ‘Monosomy 18’ at low significance was diagnosed both times. Three of the eight probes for chromosome 18 turned out to be located outside the deletion and had ratios in the normal range affecting the mean ratio of the chromosome. Subsequently, exact probe locations have been included in the automatic analysis showing the order of the probes along each chromosome. Hereby, deletions or duplications including only some of the probe sequences may be detected by inspection of ratios for individual probes.
The replies of the MLPA analyses were based on both evaluations of plots as well as automatic computer analysis. Table 2 shows that fully automatic analysis of the 1542 samples that had conclusive replies resulted in correct assignment of all analyses having appropriate quality. In total, 62 analyses had poor quality, yet no incorrect classifications of high significance were made among them. In Table 3 fully automatic analysis of the 51 samples that were replied as ‘Inconclusive’ shows that 14 analyses had in fact appropriate quality. None of these were incorrectly classified by high significance. Thus, a fully automatic MLPA analysis resulted in 1494 conclusive diagnoses with no false positive results when P⩽1.0% was used for assignments. Additionally, apart from the triple X case discussed above, no false negative results were present considering that our automatic MLPA analysis is not expected to detect mosaics (eg 45,X(24%)/46,XY) or partial deletions (46,XX,del(18)(q21 → qter)) with high significance. The vast majority of the ‘Poor quality’ cases in Table 2 and 3 were performed during the first 6 months of the 8-months period, indicating that quality is improved along with experience.
As the main indication for prenatal diagnostics is currently changing from maternal age to increased risk of aneuploidy based on ultrasound and serum analyte screening, there is an urgent need for rapid, robust, simple and yet reliable methods for diagnostic aneuploidy testing. In our hands the MLPA aneuploidy method combined with computer-assisted data analysis fulfilled these requirements. In a diagnostic routine setting where abnormal findings lead to clinical action, false positive results are unacceptable. In the present study all aneuploidies detected by MLPA were confirmed by subsequent G-banding analysis. Thus, with suitable quality criteria for the automatic data analysis and a proper P-value (currently P⩽1%) as diagnostic threshold for aneuploidy, a satisfactory sorting out of abnormal samples is provided.
Contamination of amniotic fluid by maternal blood may cause false negative results. For samples that cannot be excluded because of visible contamination, the automatic analysis may suggest contamination if the foetus is a male. According to the present data, maternal contamination is a minor problem and any misdiagnosed cases related to this circumstance will eventually be revealed in the G-banded karyotype.
In conclusion, the present data show that automatic computer-assisted MLPA is a reliable method for detection of aneuploidies. Only 3.2% of the cases were inconclusive and this figure is likely to decrease in the future as the 8-month period was initially characterized by our inexperience in both performing the practical part of the method and evaluating the results.
References
Hultén M, Dhanjal S, Pertl B : Rapid and simple prenatal diagnosis of common chromosome disorders: advantages and disadvantages of the molecular methods FISH and QF-PCR. Reproduction 2003; 126: 279–297.
Schouten JP, McElgunn CJ, Waaijer R, Zwijnenburg D, Diepvens F, Pals G : Relative quantification of 40 nucleic acid sequences by multiplex ligation-dependent probe amplification. Nucleic Acids Res 2002; 30: e57.
Slater HR, Bruno DL, Ren H, Pertile M, Schouten JP, Choo KHA : Rapid, high throughput prenatal detection of aneuploidy using a novel quantitative method (MLPA). J Med Genet 2003; 40: 907–912.
Crane JP, Cheung SW : An embryogenic model to explain cytogenetic inconsistencies observed in chorionic villus versal foetal tissue. Prenatal Diagn 1988; 8: 119–129.
Acknowledgements
We thank Inger Johannesen, Elsebeth Stensgaard and Bodil Mogensen for technical assistance.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Gerdes, T., Kirchhoff, M., Lind, AM. et al. Computer-assisted prenatal aneuploidy screening for chromosome 13, 18, 21, X and Y based on multiplex ligation-dependent probe amplification (MLPA). Eur J Hum Genet 13, 171–175 (2005). https://doi.org/10.1038/sj.ejhg.5201307
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.ejhg.5201307
Keywords
This article is cited by
-
Application of a target array Comparative Genomic Hybridization to prenatal diagnosis
BMC Medical Genetics (2010)
-
Rapid aneuploidy detection with multiplex ligation-dependent probe amplification: a prospective study of 4000 amniotic fluid samples
European Journal of Human Genetics (2009)
-
Multiplex ligation-dependent probe amplification versus karyotyping in prenatal diagnosis: the M.A.K.E. study
BMC Pregnancy and Childbirth (2008)
