
Key Points
-
The results of the UK 2003 Child Dental Health Survey confirm the trend of improved dental attendance patterns shown by previous studies, such as younger age at first visit.
-
Over 80% of children reported regular attendance, most using the General Dental Service, though there are still differences by social class.
-
Around 10% reported some problems in accessing dental care and the proportion of young children reported to have experienced extractions and general anaesthesia is still of concern.
Key Points
Children's Survey
-
1
The dentinal caries experience of children in the United Kingdom, 2003
-
2
Non-carious tooth conditions in children in the UK, 2003
-
3
Patterns of care and service use amongst children in the UK, 2003
-
4
Oral health habits amongst children in the United Kingdom in 2003
-
5
The reported impact of oral condition on children in the United Kingdom, 2003
-
6
The orthodontic condition of children in the United Kingdom, 2003
Abstract
Background The 2003 Children's Dental Health Survey is the fourth of the 10-yearly surveys of children's oral health in the United Kingdom.
Aim To detail the reported experience of dental services and dental treatment amongst children in the UK.
Method A self-completion questionnaire was distributed to a 50% sub-sample of parents or carers of the children who were clinically examined in the 2003 UK Child Dental Health Survey. This included questions relating to parental and child experience of dental services and dental treatment.
Results The proportion of UK five-year-olds reported as not having visited the dentist fell from 14% in 1983 to 6% in 2003 and the proportion reported as having visited the dentist before the age of two rose from 7% in 1983 to 31% in 2003. Over 80% of all children were reported to seek regular dental check-ups. Around 10% were reported to have had some difficulty in accessing NHS dental care while 5% of five-year-olds were reported to have experienced a general anaesthetic for dental procedures in 2003. Dental attendance was associated with social class and mothers' reported attendance patterns.
Conclusions In line with previously reported trends, the 2003 survey of children in the United Kingdom shows improvements in several areas but some aspects of attendance pattern continue to be associated with social class and mothers' attendance pattern. It is of concern that 10% of five-year-olds reported having experienced extractions and 5% general anaesthesia for dental treatment.
Similar content being viewed by others
Introduction and background
The national surveys of child dental health provide a 10-yearly summary of the condition of children's teeth in the UK and some socio-demographic variables known to be associated with oral health. This is the fourth in the series, which started in 1973.1 The series allows not only a cross sectional snapshot of the oral health of the nation's children and the factors associated with it, but also an indication of long term trends. Since the initial 1973 survey in England and Wales, the oral health of children in the UK has shown substantial change, as have reported attitudes and behaviours. This paper describes the reported use of dental services and reported experience of dental treatment and describes how these have changed since previous surveys. Questionnaire data allow us an insight into past experience of dental treatment and dental services that might not be observable from a clinical examination. For example, a child may have experienced restorative treatment in primary teeth that have exfoliated by the time of the clinical examination, leaving the appearance of a child who has never received such care. Another example would be where a child has experienced the extraction of primary teeth, but is old enough at the time of examination for the permanent successor to be present, again leaving the appearance of a child who has never experienced extractions. It is important to bear in mind that the data are reported by survey respondents, who are the parents or carers of the children, and they may be asked to recall events from some years previously. The continuity of some questions across surveys allows us to track likely changes in behaviour and attitudes over time. New issues also require exploration and therefore new questions were also added to the 2003 questionnaire.
Regular dental attendance is recommended for children in order to allow for one to one preventive advice and techniques to be employed and to allow early disease to be detected and if necessary treated.2 A shorter recall interval is recommended for children with higher risk for disease than for those at low risk2,3,4 and children should ideally first attend the dentist before their first birthday.4 The 2004 National Institute for Clinical Excellence (NICE) guidance on dental recall5 recommends that children should be seen no more frequently than three-monthly intervals and no less frequently than once a year, the individual's recommended recall interval being determined by an assessment of risk for new disease and the patient or carer's attitude to dental care. Dental attendance has been explored in the national child surveys since the first in 1973.1 and has consistently been associated with oral health and attitudes to dental care.6 Dental services for children have undergone major reform since 1983 with policy designed to make National Health Service (NHS) General Dental Services (GDS) the principal provider of child dental care through the introduction of capitation in the 1990 GDS contract and directives to salaried primary care dental services to pass patients on to GDS dentists.7,8,9 National policy has driven the provision of general anaesthesia for dental care into hospitals10,11 and more recently there have been service availability issues in many areas through workforce shortages and a move by many dentists to private arrangements.12 In addition, the distribution of child registrations and spend on child dental care under NHS GDS arrangements in England is skewed in favour of more affluent communities.13 The data from the 2003 survey, presented here, provide an insight into service use against this backdrop of multiple influences of provision and attitudes to dental care.
Survey methods and response
The 2003 survey was based on a representative sample of children five, eight, 12 and 15 years of age, attending government-maintained and independent schools in the UK. Over-sampling was undertaken for Wales and Northern Ireland to allow reporting of data for these countries individually. The survey involved 557 primary schools and 132 secondary schools. A total of 12,698 children were sampled from participating schools and asked to take part in a dental examination at school. In total 10,381 children were examined, a response rate of 82%. Schools were unable to release the home addresses of the sampled children, in compliance with the Data Protection Act. Questionnaires were therefore sent to the participating schools in stamped envelopes for the school to address and post to the parents/carers of the selected examined children. Two reminder questionnaires were sent to non-respondents, again via the school. A slip was included with the reminder questionnaires offering parents/carers the option to have a telephone interview instead of completing the questionnaire or to phone for assistance with completing their questionnaire. One telephone interview was carried out on request. Questionnaires requesting information on the child's experience of dental services and dental treatment were sent to the parents or carers of a random sub-sample of 5,480 examined children.
The questions relating to patterns of care and service use had been included in previous surveys since 19731 There were nevertheless some changes in the 2003 survey. A new socio-economic status measure (NS-SEC)14 was included, although it was still possible to derive established social class according to the older 'Registrar General's' categories as well, in order to maintain backward compatibility with earlier surveys. Previous national child surveys used a formula to classify children as 'regular', 'occasional' or 'in trouble attendees'. 'Regular' attendees were those who had visited the dentist in the six months prior to the survey and who had done so for a check up. 'Occasional' attendees were categorised as those whose last visit was longer than six months ago, but was also for a check up. Those whose last visit was because they had trouble with their teeth, or in the case of children because the community or school dentist had advised it, were classified as attending only with trouble. In the 2003 survey a direct question compatible with that used in the adult series of UK dental surveys was added which asked parents if their child usually goes to a dentist for a regular check-up, an occasional check-up or only when their child has some trouble with his or her teeth. A question concerning the parent's perception of their child's anxiety about attending a dentist was also included for the first time since the 1973 study.
In view of the complexity of the sampling design and resultant weighting procedures, sampling errors were quantified using the statistics programme STATA, and were calculated using a design factor (deft) to take account of the complex sampling and weighting procedures. The statistical significances of differences in means and percentages between sub groups were tested by calculating the confidence interval for the differences observed, based on the standard errors calculated using the design factor. This ensured that sampling error was taken into account in the testing procedure. Where statistically significant differences between groups are reported, the 5% threshold (p < 0.05) was used.
Further details of sampling, response, examination protocols and statistical methods can be found elsewhere.15
Results
Questionnaire response
The survey questionnaire was distributed to half of the sample who were clinically examined as part of the survey. Questionnaires were sent to 5,480 children from whom 3,342 questionnaires (61%) were finally returned. The overwhelming majority of the questionnaires that were returned were completed by the parents of the participants (91%) with help from the participant in a further 9% of cases.
Dental attendance Age at first visit
The majority of children were reported as having visited the dentist at least once. Table 1 shows the proportion of UK children who were reported as never having visited the dentist across the three UK surveys undertaken in 1983, 1993 and 2003 according to their age and social class. A higher proportion of five-year-olds were reported as not having visited the dentist compared with older age groups. The proportion of UK five-year-olds reported as not having visited the dentist fell from 14% in 1983 to 6% in 2003 (p < 0.05). Differences by social class still persist however and were greater in 2003; 11% and a factor of 6.5 between the least and most deprived five-year-olds in 2003 (p < 0.05) compared with 8% and a factor of 1.8 in 1983 (p ≥ 0.05).
There were few differences between individual countries in 2003, in contrast to the 1983 survey. For example 7% of five-year-olds in England were reported to have never visited the dentist in 2003, compared with 4% in Northern Ireland (p ≥ 0.05) whereas in 1983 the proportion was 13% for England and 29% for Northern Ireland (p < 0.05). The substantial reduction in the proportion of five-year-olds in Northern Ireland who were reported to have never visited the dentist between 1983 and 2003 took place between 1983 (29%) and 1993 (5%, p < 0.05) rather than between 1993 and 2003 (4%, p ≥ 0.05). Among children in England, for whom data going back to 1973 are available, 29% of five-year olds were reported as never having visited the dentist in 1973 compared with 7% in 2003 (p < 0.05).
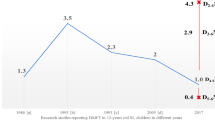
Table 2 shows the reported age at first dental visit for UK children from 1983 to 2003. This may be a difficult question for parents of older children, or the children themselves, to answer and the results should be interpreted with caution. The proportion of UK five-year-olds reported as having attended the dentist before the age of two in this latest survey (31%) has doubled from 1993 (15%, p < 0.05) and quadrupled from 1983 (7%, p < 0.05). A similar trend is apparent among eight-year-olds. Just over half of five-year-olds were reported to have visited the dentist before the age of three years in 2003 compared with just over a quarter in 1983 (p < 0.05). Among 15-year-olds nearly three-quarters were reported to have visited the dentist before the age of five years in this survey, compared with just over half in 1983 (p < 0.05). In the 2003 survey, 22% of 15-year-olds were reported to have visited the dentist before the age of two years, whereas 15% of five-year-olds were so reported in 1993 (p < 0.05), despite the data referring to the same age cohort.
Table 3 shows how the age at first visit was associated with mothers' reported attendance patterns. For example 92% of five-year-olds whose mothers reported that they attended for regular dental check-ups were reported to have visited the dentist before the age of five, compared with 55% of those whose mothers reported that they only attended when experiencing symptoms (p < 0.05).
Attendance pattern
Using rules devised for the previous UK surveys of children, attendance patterns of the children were derived from information given about the length of time since the last dental visit and the reason given for that visit. Table 4 shows the proportion of children in these categories by age group. The majority of children in all groups were classified as 'regular attendees' by these rules, around 60%, which is similar to the findings of the 1993 study. The derived attendance pattern varied by social classification, most apparently in the five-year-olds where 39% of those from routine and manual NS-SEC households were judged to be symptomatic or 'in trouble attendees' compared with 25% of those from managerial and professional households (p < 0.05). Similarly there was an association with the reported attendance pattern of the children's mothers, even in the older age groups. For example only 34% and 36% of 12 and 15-year-olds, whose mothers' attendance behaviour was to attend only when they had some trouble with their teeth, were judged to be 'regular attendees' compared with 73% and 71% respectively of those whose mothers' behaviour was to attend for regular check-ups (p < 0.05).
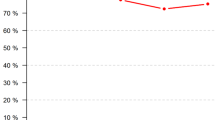
The parents or carers of the children were also directly asked in this latest survey whether their child usually went for regular check-ups, occasional check-ups or only when they had some trouble with their teeth. Over 80% of children in each of the four age groups were reported to attend usually for regular dental check-ups (Table 5). This new question in the 2003 children's survey is compatible with the question used in the 1978, 1988 and1998 national adult surveys. In 2003 the proportion of 15-year-olds reported to attend the dentist regularly was 86%, whereas the proportion of adults aged between 16 and 25 years reported as regular attendees in 1998 was only 48% and this had changed little since 1988 (45%) and 1978 (44%).
A comparison of the derived and directly reported attendance pattern is shown in Table 6. There was a high level of agreement between the two measures for regular attendance; 96% of those categorised as 'regular attendees' using the derived variable were similarly reported by respondents. There was however less agreement for the other categories; 75% of those categorised as 'in trouble attendees' by the previously used system were reported usually to seek regular dental-check-ups by their parents or carers.
Of those children who reported having visited a dentist, nearly all (98%) were reported to have last visited the dentist in the previous two years, excluding visits to an orthodontist, over 90% reported a visit within the previous year and around 80% within the previous six months, there being few differences between age groups. The reported initiating reason for the most recent dental visit is shown in Table 7. The majority of children, between 82% and 89%, in all age groups were reported as last attending for a check up or in response to a reminder from the dentist and there were few differences between the four age groups for other responses. The proportion of children who were reported as last visiting because of symptoms was higher for five and eight-year-olds in routine and manual households (15% and 18% respectively) compared with those from managerial and professional households (8% and 10%), but the differences were not statistically significant.
Dental service used and experience of treatment
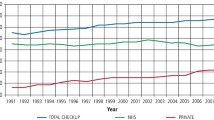
The majority of children were reported to use the General Dental Services, either in isolation or in combination with salaried primary care dental services (Table 8). There were few differences between different socio-economic groups. Few children were reported as having used services outside the NHS. Dental services for children are free under NHS arrangements and respondents were asked whether the child had ever received dental treatment that was paid for. In keeping with previous years, few respondents reported children having dental treatment that was paid for; around 1% of five-year-olds rising to 6% of 15-year-olds. While it is difficult to make comparisons with previous years due to changes made in the questions to reflect changes in service arrangements, there was consistent use of the GDS between 1983 and 1993 and this has been confirmed in the 2003 results. For example, in 1983 76% of 15-year-olds were reported as having used GDS, either alone or in combination with other services and 59% reporting using only the GDS. By 1993 this was 77% and 62% respectively. In 2003 90% of 15-year-olds were reported as having used the GDS but only 52% reported only using the GDS.
Respondents were asked whether they had ever experienced difficulty in accessing NHS dental care for their child and whether this difficulty was in the past or was current. Around 10% of children in all age groups were reported as having experienced some difficulty (Table 9) but in around three quarters of cases this was past difficulty, rather than current problems, indicating that difficulties had been overcome. Some respondents reported that dentists would only take on children for NHS dental care if the parents were private patients. Of those children for whom current difficulty was reported, 43% were reported to have visited a dentist within the previous six months and 74% within the previous year. Of those for whom difficulty was reported in the previous two years, but not currently, 77% were reported to have visited a dentist in the previous six months and 91% in the previous year.
The majority of children, around 75%, were reported as not being anxious about attending the dentist and fewer than 3% reported severe dental phobia. Most children, over 90%, were reported to have been accompanied by a parent or guardian at their last visit, even among 15-year-olds.
Table 10 shows the proportion of children who were reported to have visited a dentist but never to have experienced an extraction or a filling. The proportion of children who have not received such care has risen since 1993 in all age groups, though the change is smaller in five and eight-year-olds. The proportion of 12-year-olds who were reported to have visited the dentist, who were reported to have experienced fillings or extractions, rose from just under a quarter in 1993 to nearly half in 2003 (p < 0.05). In 2003, children from non-manual households were more likely to have visited but not had extractions or fillings, apart from 12-year-olds where the association was less clear. Around 10% of five-year-olds were reported to have experienced an extraction, this having changed little since 1983. Around a quarter (23%) of eight-year-olds in 2003 who had visited the dentist were reported to have experienced extractions, fewer than in 1993 (31%) and 1983 (42%, p < 0.05). In 2003, 12-year-olds in England who had visited the dentist were less likely to have been reported to have experienced extractions (34%) compared with Wales (58%) and Northern Ireland (53%, p < 0.05). Children in England were least likely to report fillings in all age groups and, as in 1993, the differences between England and other countries were greater in older age groups. These data are summarised in Figure 1 which illustrates an encouraging increase in children who have visited the dentist and not required treatment but also illustrates that the rate of change was slower between 1993 and 2003 compared with that between 1983 and 1993.
Respondents were asked whether the child had ever had a general anaesthetic for dental procedures. In 1983 and 1993 the questionnaire linked general anaesthesia to extractions only; in 2003 the questionnaire asked about general anaesthesia for any dental procedure. This means that the 2003 data are more comprehensive but cannot be directly compared with previous surveys, though the 2003 figures will tend to produce a higher estimate and so not under-report the experience of general anaesthesia compared with previous surveys. The reported lifetime experience of general anaesthesia for dental procedures in 2003 was 5% among five-year-olds, 11% among eight and 12-year-olds and 21% among 15-year-olds. By comparison 7% of five-year-olds, 27% of eight-year-olds, 35% of 12-year-olds and 47% of 15-year-olds in England and Wales were reported to have experienced general anaesthesia for extractions in 1983. If one assumes that the majority of experience of general anaesthesia for dental procedures in children is for extractions then it would seem that an additional 14% of 15-year-olds had experienced a general anaesthetic between the age of five (7% in 1993) and 15 (21% in 2003).
Discussion
The response rate in 2003 was lower than that for the 1993 survey, reflecting the different methodology adopted to distribute questionnaires to parents and carers. The weighting methodology adopted however was designed to compensate for non-response bias.15 The problems inherent in interpreting reported data are illustrated by the finding that in 2003 nearly a quarter of 15-year-olds were reported to have visited the dentist before the age of two years, whereas in 1993 only 15% of this age cohort, then aged five years, were reported to have visited before that age. However, the tracking of responses to the same questions over time gives us an indication of how people's behaviour is changing. In addition it may also give us an indication of people's changing attitudes to an issue, given that respondents may well want to give an answer in keeping with what they think they should have done, if not truly representing what they actually did do.
The results of this study confirm an ongoing trend of children being first taken to the dentist at an earlier age. This is shown by a falling proportion of children aged five years who were reported never to have seen a dentist compared with previous surveys and an increasing proportion of children who were reported to have first visited the dentist before the age of two years. Nevertheless, in 2003 less than a third of five-year-old children were reported to have visited the dentist before the age of two years, which falls far short of the recommendations of the British Association of Paediatric Dentistry.4
While it would appear that children are being first taken to the dentist at an earlier age than previously, the results of this study do not show an increase in the proportion who attend 'regularly', which remains at around 60% using the method to determine 'attendance pattern' that has traditionally been used in national surveys of children. The formula used to calculate the derived attendance pattern is problematic as it is based entirely on the timing and circumstances of the last dental visit as a means to determine habitual behaviour. While the derived 'attendance pattern' variable enables comparison with previous studies, its dissonance with the directly reported attendance pattern is of concern, as is the fact that it is not compatible with that used in the surveys of UK adults. It is interesting that in this survey the proportion of 15-year-olds reported as usually attending for regular dental check-ups, according to the question compatible with adult surveys, is almost double the proportion of 16 to 24-year-olds reported as attending for check-ups on the same basis, according to the identical question used in the UK surveys of adults. Either this indicates that there has been a dramatic change towards increased attendance among young adults, which will become apparent in the 2008 adult survey or, more likely, there is a marked deterioration in attendance in early adulthood. In considering this issue it is notable that a high proportion of 15-year-olds were reported to have been accompanied at their last visit to the dentist. Encouragingly, over 90% of children were reported to have visited a dentist in the previous year, in line with the recent NICE guidance on maximum recall interval for children, though it is not known whether those at highest risk of developing new disease were attending as frequently as they should. The guidance was issued after the survey took place so it seems that in most cases this standard is already being met for children.
Defining what is NHS dental care and establishing what type of services have been used is always problematic, given the complexity of services and differing perceptions of what constitutes NHS dental care. The results of this study indicate a continued major role for the general dental services by 2003 and do not indicate that there were insurmountable difficulties in accessing NHS dental care by children, as most parents who reported recent problems with access to NHS dentistry also reported that their child had attended for dental care within the last six months.
The picture of reducing experience of dental caries, as evidenced by reduced reporting of experience of extractions in younger children and fillings in all children is encouraging, though the rate of reduction appears less between 1993 and 2003 compared with 1983 to 1993. Despite these reductions a high proportion of children were still reported to have experienced extractions; 10% of five-year-olds and nearly a quarter of eight-year-olds. In addition 5% of five-year-olds in 2003 were reported to have experienced a general anaesthetic for dental procedures. The marked difference between the proportion of eight and 12-year-olds (11%) who have experienced a general anaesthetic compared with 15-year-olds (21%) is potentially some cause for concern. Those children who were 15 in 2003 would have been 10 in 1998 when the revised General Dental Council Guidance10 on general anaesthesia was issued and around 13 to 14 by January 2002 by which date all provision of dental treatment under general anaesthesia had moved to hospitals.11,16,17 By comparison those children who were 12 in 2003 were aged around seven in 1998 and 10 to 11 by January 2002; eight-year olds in 2003 would have been aged three in 1998 and around six to seven by January 2002. It might be expected that the relatively high figure for 15-year-olds was primarily the result of general anaesthesia provision between the age of seven and 10 years, before the main impact of legislative changes was felt, presumably for the extraction of carious primary teeth and possibly some orthodontic extractions. If this is so then the 12-year-olds in 2003 might be expected to have had extractions managed mostly under local anaesthetic as the service arrangements were changing by the time they needed this treatment. Alternatively it could be that the difference is mainly due to orthodontic extractions between the age of 10 and 12 which were carried out under a general anaesthetic for those children who were 15 in 2003. This would assume however that orthodontic extractions under general anaesthesia were still commonplace after 1998, which would not have been in keeping with the spirit of the GDC guidance.
In addition, it is of concern that attendance before the age of five and attendance for check-ups continue to be associated with relative affluence and with mothers' attendance patterns. Therefore the children in society who are most likely to experience dental disease would seem to be less likely to access care.
Conclusions
Surveys of dental health undertaken in the United Kingdom generally show a pattern of improvement from one survey to the next. The 2003 survey of children in the United Kingdom also shows improvements in areas such as the reported experience of dental treatment and the age when children first attend a dentist. Some aspects of attendance pattern continue to be associated with social class and mothers' attendance patterns. Service access for children is a reported problem but it would appear not to be an insurmountable problem for many parents who, despite reporting access problems, also reported that their child had attended a dentist within the six months prior to the survey. The survey also found that 5% of those born in the last five years have already experienced a general anaesthetic in order to undergo dental procedures for conditions that are largely preventable.
References
Todd JE . Children's dental health in England and Wales 1973. London: HMSO, 1975.
Levine RS, Stillman-Lowe CR . The scientific basis of oral health promotion. London: British Dental Association, 2004.
Nunn J, Crawford PJ, Page J, Winter G . British Society of Paediatric Dentistry: A policy document on the dental needs of children. Int J Paed Dent 1997; 7: 203– 207.
Crawford PJM . UK national clinical guidelines in paediatric dentistry. Continuing oral care: review and recall. Int J Ped Dent 1998; 8: 227– 228.
National Institute for Clinical Excellence. Clinical Guideline 19. Dental Recall: Recall interval between routine examinations. NICE 2004. www.nice.org.uk
Hawley GM, Holloway PJ, Davies RM . Dental health status associated with documented dental attendance patterns in adolescents. Comm Dent Health 1997; 14: 22– 24.
Promoting Better Health. The government's programme for improving primary health care. Cm249. London: HMSO, 1987.
Department of Health 1989. Health services management. The future development of Community Dental Services. Circular HC(89)2
Department of Health 1989. Future of the Community Dental Service. Professional Letter PL/CDO(89)2
General Dental Council. Maintaining Standards: Guidance to dentists on professional and personal conduct. Revised November 1998. London: General Dental Council.
Department of Health. A conscious decision. A review of the use of general anaesthesia and conscious sedation in primary dental care. Report by a Group chaired by the Chief Medical Officer and Chief Dental Officer. London: Department of Health, 2000.
National Audit Office. Department of Health. Reforming NHS dentistry: Ensuring effective management of risks. London: The Stationary Office, 2004.
Landes DP, Adams GC, Whiston S . Distribution of NHS resources for children's dental care in general dental practice in England. Comm Dent Health 2004; 21: 149– 154.
Rose D, Pevalin DJ(Eds) . A researcher's guide to the National Statistics Socio-economic Classification. London: Sage Publications, 2003.
Pendry L, Lashkari G, Bewley H . Technical report: 2003 children's dental health survey. London: Office for National Statistics, 2004.
Robinson H . General anaesthesia for dental treatment (DoH letter to dentists and health authorities 15/2/01)
Winterton R . Written Response. Commons Hansard 23 Oct 2003: Col. 732W
Acknowledgements
This work was undertaken by a consortium comprising the Office for National Statistics and the Dental Schools of the Universities of Birmingham, Cardiff, Dundee and Newcastle and the Dental Health Services Research Unit, Dundee who received funding from the United Kingdom Departments of Health; the views expressed in this publication are those of the authors and not necessarily of the Office for National Statistics or Departments of Health.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed paper
Rights and permissions
About this article
Cite this article
Morris, A., Nuttall, N., White, D. et al. Patterns of care and service use amongst children in the UK 2003. Br Dent J 200, 429–434 (2006). https://doi.org/10.1038/sj.bdj.4813462
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4813462
This article is cited by
-
Impact of dental visiting patterns on oral health: A systematic review of longitudinal studies
BDJ Open (2024)
-
Trends of dental caries in permanent teeth among 12-year-old Chinese children: evidence from five consecutive national surveys between 1995 and 2014
BMC Oral Health (2021)
-
Clinical leadership and prevention in practice: is a needs led preventive approach to the delivery of care to improve quality, outcomes and value in primary dental care practice a realistic concept?
BMC Oral Health (2015)
-
Initial management of paediatric dento-alveolar trauma in the permanent dentition: a multi-centre evaluation
British Dental Journal (2010)
