
Key Points
-
This paper evaluates the development of primary dental care by the four first wave personal dental services (PDS)pilots which introduced locally agreed remuneration arrangements for adult care based on capitation funding.
-
On the basis of limited data, the pilots were found to have promoted a less interventionist approach to care by participating dentists compared with historical GDSactivity, and provided an incentive to care for additional patients.
-
The experience of these pilots provides a basis for developing a capitation funding model for adult primary dental care.
Abstract
Since 1948, incentives associated with the remuneration of general dental practitioners (GDPs) have remained largely unaltered for the care of adults. In 2000/01, 89% of GDPs' gross income relating to adult patients came from fees for over 400 items of service.1 The direct 'treadmill' link between income and items of treatment provided has been long recognised: in 1964, the Tattersall report declared that 'there is no future for the profession, or indeed for general dental practice as an art and a science, in the system of remuneration as presently operated'.2 Tattersall et al. outlined an alternative system of remuneration based on capitation payments with an element of fee-for-service payments for complex treatment. Nearly 20 years later, Gordon3 eloquently stated the argument for change: 'What is required is a fundamental change in the system of dental remuneration. To go from the Scylla of item of service (over-prescribing) to the Charybdis of capitation (supervised neglect) at least has the advantages that it can be monitored and policed in a far more effective manner'.
Similar content being viewed by others

Main
While child capitation was promoted,4,5 piloted6 and implemented in the 1990 'New Contract',7 views on adult capitation remained more cautious.8 After a number of developments in the 1990s,9,10,11,12,13,14 15 first wave personal dental services (PDS) pilots were approved to commence from October 1998. The PDS regulations provided an opportunity for GDPs to experiment with capitation-based funding of adult general dental services.
Evaluation of the capitation-based PDS pilots
This paper focuses on the four pilots formed by GDPs wishing to provide general dental services using remuneration arrangements based on capitation for adult patients, and forms part of a wider evaluation of first and second wave PDS pilots funded by the Department of Health.15,16,17 Qualitative data on each pilot were collected from the pilot lead and health authority lead in semi-structured face-to-face interviews held between February and April in 2000 and 2001. The pilots' contracts and annual reports to the Department of Health were examined. Additional data collection took place as part of the wider evaluation.17
Activity data relating to the four capitation-based pilots and GDS activity in the host health authorities were supplied by the Dental Practice Board for England and Wales (DPB). Some baseline data were problematic due to difficulties relating to contract number changes following the change from GDS to PDS. Treatment data for the year in which the pilots started, 1998/99, have not been used because of data quality issues.
Pilot characteristics
The four capitation-based pilots varied considerably (Table 1). While both pilots A and B were located in small rural towns, pilot A aimed to provide comprehensive care for the entire local population, pilot B focused on adults only and included a quarter of the practices in the locality. Pilots C and D both operated in deprived urban locations and shared a stated focus on children with unmet needs while also including adults.
Main objective of the pilots
All four capitation-based pilots had objectives to increase access to routine dental care. Pilots A and B both aimed to improve access in response to a high level of demand for care, and their objectives were expressed as targets to increase the number of registered patients. Pilots C and D both experienced low levels of demand from high needs populations and did not specify targets for registration increases.
Capitation-based contracts
Each pilot was the product of local negotiation between the host health authority and a number of principal dentists, referred to as 'providers' in the resulting contracts. Local contract development was subject to two criteria. First, the provider dentists had to be funded at a level that at least matched their pre-pilot GDS income in return for a similar level of service. Second, patients treated in any pilot would continue to be charged the same patients' charges as would apply within NHS GDS. The local funding arrangements are outlined below:
Pilot A: A 'baseline' payment was paid to each of the providers by the health authority. The baseline payments were set at a level which would match the historical GDS non-patient fee income of the providers. Net increases in the number of registered patients attracted annual 'growth' payments of £50 for children and exempt patients and £30 for fee-paying patients. Growth payments were initially calculated for each six-month period, and later calculated on a monthly basis. The higher rate for growth payments to exempt patients compared with fee-paying patients was intended to balance the financial reward of treating these two patient groups over a period of about four years. Non-provider dentists working in the pilot were paid on a fee-per-item basis by the practice-owning providers.
Pilot B: This pilot was limited to adults. For newly registered patients, fees per item of treatment were payable, at the GDS rates, for the first course of treatment provided. All the dentists working in the pilot had provider status. Monthly capitation fees became payable on completion of the first course of treatment. Three levels of the capitation payments were initially used. Payments for patients with some natural teeth were at a rate equivalent to an annual payment of £29.76 and, until April 2002, higher and lower level payments were used for high need and edentulous patients respectively. The higher and lower level payments were discontinued because they were reported to be little used and administratively cumbersome. The capitation payments were subject to bi-annual review and covered a specified range of common treatments. All payments made to the pilot were net of patient charges collected. In April 2002, the registration period was extended to two years in order to encourage an increase in the time between inspections.
Pilot C: The level of the capitation payments was age-related and equivalent to annual payments ranging from £16.92 for children aged up to two, to £50.88 for children aged 13 to 17. The capitation payments were made on a monthly basis and covered a specified range of common treatments. Some activity attracted fees per item of treatment in line with the GDS payment schedule. Endodontic treatment and complex periodontal treatment were paid at the GDS rates plus 10%.
Pilot D: In addition to setting baseline payments to match the historical income of the providers under the GDS regulations, the level of growth payments for additional registrations was initially set to match the historical GDS income. This resulted in practice-level annual growth payments varying from £46 to £70 per additional registration. From September 2000, 70% of the funding per registration was set at the same level across all the practices in the pilot, and 30% was weighted by the Jarman score, based on the location of the patient's residence. This approach resulted in an average annual payment of £63 per registration (range £60 to £64). Funding was calculated using registration data on a monthly basis. The non-provider dentists in this pilot were funded through a range of mechanisms from salaried to capitation or a mixture of capitation and fee-per-item. In addition, some of the pilot's activity was carried out by salaried staff seconded from the community dental service.
Access to primary dental care
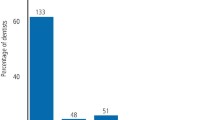
The capitation-based pilots expressed their aims to increase access in terms of registrations, which was therefore a key measure for these pilots. Figure 1 shows the change in registrations between the quarters ending December 1998 and June 2001.

Change in total patient registrations for the four capitation-based pilots
Pilot A: The initial target was to increase registrations by up to 15% per annum. The number of registrations increased by 14% between December 1998 and September 1999. Further increases were not realised and the pilot forecast a 4% increase in net registrations in 2001/02. The health authority lead for the pilot reported that the pilot had achieved its objective to 'provide unhindered access to NHS dental services to the residential population'. Complaints by members of the public to the health authority about the unavailability of NHS dentists in the locality were reported to have ceased. The overall increase in registrations to March 2001 was limited due to one of the nine providers leaving the pilot in early 2001 (see below).
Pilot B: The pilot's initial target was to increase registrations by 18% between October 1998 and March 2000, and it experienced an increase of 9% over this period. The target increase for 2000/01 was 11%, and it experienced an increase of 4% over this period based on data presented in the pilot's annual report, or 2% based on DPB data. The pilot's 2000/01 annual report stated that there were no availability problems in the designated area, and so the pilot had 'completely' reached its target population.
Pilot C: This pilot did not set specific targets for registrations although an increase in registrations was an objective, particularly for children. The pilot experienced a reduction in the number of participating dentists and this accounts for an overall reduction in registrations of 34% between December 1998 and March 2001. However, the number of child registrations increased by 29%, and the number of adult registrations increased by 1% during this period, for dentists who remained in the pilot.
Pilot D: The pilot did not report registration targets, although, as with pilot C, increasing registrations for children was a particular objective. This pilot experienced the largest increase in registrations. This is in part due to the pilot increasing the registration period from 15 to 24 months. The number of child registrations increased by 45% and the number of adult registrations increased by 30%, between December 1998 and March 2001. The dip in registrations in the quarters ending September 1999 and September 2000 was reported by the health authority lead to be due to vocational trainees leaving post and their patients not being immediately re-registered.
Activity measures
Some insight into the pattern of treatment provided by these pilots is provided by comparing the PDS activity provided by each pilot with the GDS activity provided by those dentists who subsequently went into the pilot. In order to facilitate a 'like for like' comparison, the DPB provided the evaluation team with a set of activity data for these pilots in 1999/00 and 2000/01 which were processed using the GDS regulation criteria. This approach means that any activity provided by the PDS pilot that would not have accrued a fee under the GDS regulations is excluded from the comparison. It is important to note that the incentive to collect these data is different under GDS and PDS; under the latter arrangements there was often no link between such reporting and payment, as there is under GDS.
Types of treatment
Table 2 uses data grouped into seven treatment types used by the DPB and described in Box 1. Pilots A and D shared a trend of reducing the proportion of activity classified as 'intricate work' and to increase the proportion of work classified as 'no dental intervention' (Table 2). While pilot B also shows an increase in the proportion of activity classified as no dental intervention, the proportion of intricate work was maintained. This finding is consistent with the pilot's financial incentives because intricate work attracted fee for service payments in pilot B. Pilot C experienced little change in the proportion of intricate work, but experienced a substantial move from the routine work classification to no dental intervention.

Common items of treatment
Table 3 summarises the treatment rates for the most common items of treatment for adults in the three pilots with 15 month registration periods. The table includes the GDS treatment rates in 1997/98 for the dentists that subsequently went into the PDS pilots, and the treatment rates for all dentists working in the pilots in 1999/00 and 2000/01. Treatment rates are also shown for comparator GDS activity within the host health authorities. The difference in change in treatment rates between 1997/98 and 2000/01 for each pilot and comparator was tested for statistical significance using standard probabilistic arguments and regarding the number of items of treatment as poisson random variables.
The GDS registration period for adults changed from two years to 15 months on September 1,1996. This change means that registration data for 1997/98 are inflated in comparison with registration data for 1999/00 and 2000/01, and treatment rates based on registrations will increase over time, other things being equal.
Table 3 shows that for teeth filled (one of the common items of treatment), pilots A and B experienced a reduction in treatment rates between 1997/98 and 2000/01 in contrast to increases experienced by the GDS comparators. Pilot C experienced a much larger reduction in the rate of teeth filled than its GDS comparator. The reductions in treatment rates for teeth filled were such that while in 1997/98 the dentists that subsequently went into the pilots experienced higher treatment rates than their local GDS colleagues, by 1999/00 the dentists in the PDS pilots had lower treatments rates, which were sustained in 2000/01.
Table 3 also illustrates the very wide variation in treatment rates between pilots and between other GDPs working in the four health authorities. For example, in 2000/01 the rate for teeth filled varied from 58 per 100 adult registrations in Pilot A to 318 per 100 adult registrations for the GDS dentists in pilot C's health authority.
Scaling was another common item of treatment and all three pilots experienced a reduction in treatment rates between 1997/98 and 2000/01 in contrast to increases experienced by the GDS comparators (Table 3). The three pilots also share a trend of smaller reductions or little change in rates for the three other items of treatment shown in Table 3 (teeth extracted, teeth inlayed or crowned, teeth root filled) between 1997/98 and 2000/01.
While sharing activity trends, the pilots were subject to considerable variation in the detail of the capitation funding arrangements and the payment methods for participating dentists. For example, in pilot A, while the providers (practice owners) were funded on the basis of the capitation payments outlined above, the non-provider dentists working in the pilot were paid on the basis of their activity and the GDS fee structure. For this reason, the provider and non-provider dentists did not share the same financial incentives. As expected the provider dentists experienced lower treatment rates than their non-provider colleagues. This comparison is simplistic, however, as it may be that non-provider dentists saw a higher proportion of 'new' patients (requiring comparatively high levels of treatment) than the provider dentists with their established patient lists.
Courses of treatment
The average number of completed courses of treatment in each six-month period between the six months ending September 1999 and September 2001 is shown in Figure 2. The two 'high demand' pilots (A and B) experienced a higher number of completed courses of treatment compared with the 'low demand' pilots. It is interesting that pilot C's experience is similar to pilot D's experience given that the registration period for pilot D is 24 months compared with the other pilots' registration period of 15 months.

Data reported on the monthly activity returns (MARs) produced by the DPB. The data covering the year to March 2000 have been discounted by a pilot-specific factor calculated by the DPB which is intended to account for double counting of activity data during this period due to data collection and transmission problems.
Costs
The estimated aggregate cost in 2000/01 of the three pilots that maintained 15 month registration periods is shown in Table 4. These cost data include the payments made to the pilots under the locally agreed capitation-based funding arrangements and the estimated payments made by patients (who continued to pay charges due under the GDS regulations). The patient charges may be under recorded, either because of treatment data transmission problems or a reduction in the incentive to record treatment by dentists who no longer had to record treatment in order to be paid.
The cost comparison with regional GDS activity shown in Table 4 is not straightforward for three reasons. First, the regional GDS costs provide only very limited insight into what the cost of treatment provided to the pilots' patients might have been if they had been treated under GDS arrangements. Second, a measure of cost based on registrations is unsatisfactory. For example, the cost per registration under a service which offers access to an entire local population is not comparable with one in which 'new' patients are barred. Third, the care provided under PDS and GDS is not equivalent. PDS is characterised by less intervention (particularly teeth filled) and greater reported (though not quantified) patient education. Demonstrating whether the intended improvement in oral health under PDS is realised would require detailed study over a period longer than three years. In the short term, the financial support for a less interventionist approach has provided sufficient time and incentive for PDS dentists to provide improved access to primary dental care for NHS patients.
Estimates of what the PDS activity in 2000/01 would have cost if funded under the GDS regulations, provides a further comparison (Table 4). However, for the reasons noted above, this measure is of limited value.
The impact of capitation funding on activity
The absence of many of the historical income maximising incentives associated with the GDS regulations provided an opportunity for the PDS dentists to promote a less interventionist approach to dental care. The analysis presented here indicates that the capitation-based pilots experienced changes in treatment patterns which are compatible with the new incentives.
Of the two pilots which aimed to increase access to primary dental care in response to high levels of demand for services, pilot A more clearly illustrates the potential for changing practice. Pilot A reduced the rate of teeth filled (from 81 to 61 per 100 adult registrations) and then sustained a low rate compared with local general dental practitioners. Pilot B experienced a similar, but smaller, change in practice, which is in line with its decision to maintain the GDS funding arrangements for a patient's first course of treatment. In this respect, pilot B's approach follows Tattersall's recommendation.
The 'low demand' pilots C and D also experienced changes in the pattern of care provided in line with a more preventative approach. However, these pilots differed from each other in terms of context, management and financial arrangements, and outcomes and therefore provide only a limited basis for comparison. Nevertheless, these pilots offer important insights into the challenges of providing high quality primary dental care to patients with high needs.
The less interventionist approach, combined with the availability of growth funding, contributed to the pilots' ability to treat additional patients. For example, pilot A was successful in terms of providing access to primary dental care such that complaints to the local health authority by members of the public unable to see an NHS dentist in the pilot's locality were reported to have ceased. The fact that this outcome was achieved with less than the expected increase in registrations highlights the extent to which registrations is an unsatisfactory denominator.
The move to a more preventive approach to dental care implies that GDS arrangements result in some unnecessary treatment. Similarly, dental care provided under capitation funding arrangements is open to the perverse incentive to under treat or withhold necessary treatment. One measure that sheds some light on this issue is the Dental Reference Service patient examinations. Although the number of examined patients from the pilots was small, the Dental Reference Service had not identified any systematic problems during the study period. It may be too early to assess the potential consequences of any over-zealous embracing of a 'watch and wait' philosophy. Nevertheless, one PDS pilot lead dentist emphasised that the Dental Reference Service is able to detect under treatment, because a hole that should have been filled is visible. 'On the other side of the coin, you can't demonstrate over prescription, because you can see a tooth that has got a filling in, but you don't know whether it had a hole that needed it. So you are not comparing like with like. Whilst all my patients are there and the evidence is there, the corresponding evidence for over prescription is not available.'
A further concern is the potential increase in the incentive for a PDS dentist to promote private dental treatment in comparison with a dentist offering NHS care under the GDS regulations. In the absence of routine activity data on private practice activity, this issue could not be explored. However, the pilots' health authority leads reported that there had not been any increase in patient enquiries or complaints which may have indicated a major increase in private activity. The health authority lead for one of the pilots reported that the randomly chosen inspection of 20 patients' notes during each quarterly visit to practices had not indicated any change in the level of recorded private activity.
Local contracts for primary dental care
In general the capitation-based pilots have been managed through informal contact between the health authority and pilot leads, based on a high level of mutual trust. The contracts are simplistic. Several of the more proactive health authority and pilot leads have started to develop more sophisticated contracting arrangements which begin to provide a framework for performance management appropriate for organisations as they move beyond pioneer pilot status. Many of these issues are shared by the first wave personal medical services (PMS) pilots.18 Arrangements for monitoring activity and cost need to improve in order to better manage dentists' workload when, for example, dentists join or leave a pilot. Nevertheless, the local contracts have provided a framework in which health authorities and dentists have started to address quality issues, which has great potential when compared with the GDS arrangements.
Three dentists left pilot C during 1999/00 and a further three dentists left in 2000/01. One of the nine provider dentists left pilot A in early 2001. Some departures are not necessarily related to the operation of the pilot (eg leaving after a period of maternity leave) while others illustrate issues that need to be addressed if capitation-based funding is to be successfully extended. For example, one dentist was reported to have left a pilot because they were seeing a high proportion of high-need patients requiring treatment at a level that made the local funding arrangements financially unattractive. A needs-based capitation funding formula is required to support local contracting for primary dental services.
Another dentist was reported to have left a pilot because they were 'not working towards the scheme's objectives'. The health authority lead reported that this dentist would not have met subsequently introduced acceptance criteria for dentists wishing to join the pilot, and so illustrates the greater potential of the pilots to influence practice compared with GDS.
Information technology and management information
The use of IT to electronically transfer activity and cost data between the pilots and the DPB was a feature of the first wave pilots. For some pilots this represented an opportunity to gain additional funds to update existing software and hardware, while for others it entailed computerisation and a difficult learning curve. IT problems led to the collection of basic PDS activity data being problematic. With hindsight, it is clear that the challenge associated with adapting the GDS data collection procedures was greater than initially anticipated. Data management issues would have benefited from more effective communication between the pilots, health authorities, the Department of Health and DPB. Whilst payment moved to a capitation basis, the retention of all GDS mechanisms for calculating patient charges and basic reporting of activity meant that any other data-related tasks required by the pilot for performance management represented an additional burden, and the new pilot-related information tended to suffer in consequence.
Sharing experience
The pilots could undoubtedly have learnt from each other and the absence of initiatives by the Department of Health to promote 'collaborative' learning is a feature of the PDS (and PMS) first wave, in contrast to other major pilot programmes.19 The NHS Modernisation Agency's role in taking forward the agenda set out in NHS Dentistry: Options for Change20 will facilitate opportunities to address this deficiency with the proposed field sites.
Lessons
It is impossible to determine the 'ideal' capitation model on the basis of the four pilots with their diverse funding arrangements and characteristics. Unlike the trial of child capitation,6 the PDS pilots were not set up under the auspices of a controlled clinical trial. The available routine data were limited and of variable quality and it was not possible to directly measure the oral health of patients.
Having noted this caveat, the PDS capitation-based pilots succeeded in providing an opportunity for dentists to pursue a less interventionist approach to dental care, in contrast to the incentives associated with the GDS regulations. The pilots demonstrate that the concerns expressed by Tattersall and other commentators since can be addressed. Nevertheless, local management capability is necessary if the potential of local contracting for primary dental care is to be realised. The development of dental expertise within strategic health authorities and primary care trusts (PCTs) is now a key challenge in order to secure effective leadership in the future if local commissioning is to be extended.
The pilots provide a basis for addressing a range of issues. For example, the experience of pilot A suggests that it is not necessary to fund the first course of treatment for 'new' patients using item of service payments. Similarly, the experience of pilot B suggests that associate dentists do not necessarily have to remain funded under the GDS regulations. Arrangements for managing payments flows relating to the transfer of patients, when dentists join or leave could be improved if the lessons of these pilots are acted upon.
Further analysis of problems associated with the national GDS contractual arrangements was produced by The Audit Commission in 200221 and NHS Dentistry: Options for Change20 could be viewed as a step towards replacing GDS funding arrangements. The limited experience of the capitation-based pilots suggests that this alternative is promising. However, there are a number of major outstanding issues which must be addressed. These include the development of a needs-based capitation funding formula for use across PCT populations, a related change in the role of registrations to one based on PCT populations, a review of patient charges and further research on the benefit of commonplace dental interventions to guide change.22
The capitation-based pilots illustrate the potential for dentists to change their prescribing behaviour and provide care which was commonly viewed as being to the long-term benefit of patients. Whether in response to 'high' or 'low' local demand, the pilots have enabled dentists to step off the 'treadmill' and work towards the goal of maintaining their patients' dental fitness.
References
Dental Practice Board. Gross Fees GDS Annual Statistics April 2000 – March 2001. Eastbourne: DPB, 2001.
Tattersall W, Albert D, Brackenridge J, et al. Report of the ad hoc sub-committee on methods of remuneration. Br Dent J 1964; 117: 331–346.
Gordon E Dental diagnosis and remuneration Br Dent J 1982; 153: 9.
Fit for the future. Report of the Committee on Child Health Services. (Chairman: S Court). London: HSMO, 1976.
Dental Strategy Review Group. Towards better dental health – guidelines for the future. London: Department of Health and Social Security, 1981.
Coventry P, Holloway P, Lennon M, Mellor A, Worthington H A trial of a capitation system of payment for the treatment of children in the general dental service. Comm Dent Health 1989; 6 (supplement 1): 1–63.
Mellor A, Holloway P The new capitation system. Dent Update 1991; 18: 117–120.
Schanschieff S, Shovelton D, Toulmin J Report of the committee of enquiry into unnecessary dental treatment. London: HMSO 1986.
Bloomfield K Fundamental review of dental remuneration. London: Department of Health, 1992.
Health Select Committee Fourth Report. Dental Services Volume 1; report together with the proceedings of the committee. London: HMSO, 1993.
Department of Health. Improving NHS dentistry. London: Department of Health, 1994.
Malone G Written answer (Dental Services). Hansard 5/4/95, Column 1211.
Department of Health. Choice and opportunity (Primary Care: the future) Cm 3390, 1996.
National Health Service (Primary Care) Act 1997. London: The Stationary Office, 1997.
Smith J, Baines D, Bradnock G, Morris J The PDS pilot sites: painting the picture and posing the questions. Birmingham: HSMC, 1999.
Smith J, McLeod H, Goodwin N, Morris J, Hill K, Hall A, Bradnock G, Ham C New models of NHS dental care: interim report of the national evaluation of Personal Dental Services. Birmingham: HSMC, 2000.
Hill K, Goodwin N, Morris J, Hall A, McLeod H, Burke T PDS pilots: Final report of the national evaluation Birmingham: HSMC, 2003.
Walsh N, Andre C, Barnes M, Huntington J, Rogers H, Hendron C, McLeod H . First wave PMS Pilots: opening pandora's box. Birmingham: HSMC, 2002.
Ham C, Kipping R, McLeod H, Meredith P Capacity, culture and leadership: lessons from experiences of improving access to hospital services. Final report from the evaluation of the National Booked Admissions Programme first wave pilots. Birmingham: HSMC, 2002.
NHS Dentistry: Options for Change. London: Department of Health, 2002. www.doh.gov.uk/cdo/optionsforchange
The Audit Commission. Dentistry: primary dental care services in England and Wales. London: The Audit Commission, 2002.
Davenport C, Elley K, Fry-Smith A, Taylor-Weetman C, Taylor R The effectiveness of routine dental checks: a systematic review of the evidence base Br Dent J 2003; 195: 87–9
Acknowledgements
The views expressed in this paper are those of the authors and are not necessarily those of the Department of Health which funded the evaluation. The authors would like to thank the staff in the four pilots and health authorities who gave freely of their time in enabling the authors to gather data. The authors also wish to thank the staff of the Dental Practice Board for England and Wales for supplying data.
Author information
Authors and Affiliations
Corresponding author
Additional information
Refereed Paper
Rights and permissions
About this article
Cite this article
McLeod, H., Morris, A. & Hill, K. Evaluation of personal dental services (PDS) first wave pilots: the alternative to general dental services (GDS) offered by the capitation-based pilots. Br Dent J 195, 644–650 (2003). https://doi.org/10.1038/sj.bdj.4810782
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bdj.4810782
This article is cited by
-
Managing resources in NHS dentistry: the views of decision-makers in primary care organisations
British Dental Journal (2008)
-
A qualitative analysis of the planning, implementation and management of a PDS scheme: Lessons for local commissioning of dental services
British Dental Journal (2006)
-
National evaluation of personal dental services (PDS) pilots: main findings and policy implications
British Dental Journal (2003)
