
Abstract
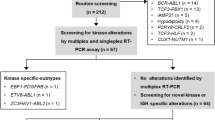
Pathological features and genomic basis of a rare case of ALK+, CD30−, CD20− large B-cell lymphoma were analyzed. A 36-year-old Japanese female was admitted because of lumbago and constitutional symptoms. Physical examination and laboratory tests showed anemia (hemoglobin, 7.5 g/dL), mild hepatosplenomegaly, and immunoglobin G (IgG) λ-type monoclonal gammopathy (IgG, 2782 mg/dL). The lymphoma spread exclusively in extranodal sites such as bone marrow, liver, spleen, ovary, and muscle. Biopsy specimens obtained from the ovary showed monomorphic proliferation of large immunoblastic cells with basophilic cytoplasm, round-shaped nuclei with a high nuclear to cytoplasmic ratio, and prominent single nucleolus. Immunostaining with anti-anaplastic lymphoma kinase (ALK) antibody, ALK1, showed finely granular cytoplasmic staining pattern. These cells were also positive for epithelial membrane antigen, CD4, CD19, CD38, CD138, cytoplasmic IgG, and λ chain, but negative for CD30 (Ber-H2), CD56, CD57, and other T- and B-cell markers. Southern blot analyses revealed that Ig heavy and λ light chain genes, but not T-cell receptor (TCR) β gene, were clonally rearranged. Chromosomal analyses by conventional G-banding, spectral karyotyping, and fluorescence in situ hybridization showed complex abnormality involving 2p23, and chromosome 2 was translocated to chromosome 17. As 2;17 translocation resulting in the fusion of clathrin heavy chain (CLTC) gene with ALK was previously reported in inflammatory myofibroblastic tumor, we performed reverse transcriptase-polymerase chain reaction and demonstrated that the lymphoma cells contained CLTC-ALK fusion transcript. Under the diagnosis of ALK+, CD30−, CD20− large B-cell lymphoma, she was treated with conventional combination chemotherapies. However, the lymphoma was primarily chemotherapy resistant, and the patient died 11 months after admission. We consider that this case confirms the existence of ALK+, CD30−, CD20− large B-cell lymphomas proposed by Delsol et al. (16) and further provides relevant information regarding their clinicopathological features and cytogenetics.
Similar content being viewed by others


INTRODUCTION
It is now well recognized that anaplastic large cell lymphoma (ALCL) with the (2, 5)(p23;q35) translocation (1, 2, 3, 4), which juxtaposes the nucleophosmin (NPM) gene on chromosome 5q35 to the ALK gene on chromosome 2p23 (5), constitutes a distinct clinicopathological entity (6, 7, 8). This rearrangement leads to the production of a novel 80-kDa fusion protein with transforming properties (9, 10), which contributes to the development of ALCL (11). Subsequent research has further revealed that translocations other than t(2;5)(p23;q35) also activate the ALK gene (12, 13, 14). Touriol et al. (15) reported a unique variant of ALCL containing the ALK gene fused to the clathrin heavy chain gene. Lymphoma cells possessing this fusion protein are characterized by an unusual granular cytoplasmic staining with anti-ALK antibody (ALK1).
Recently, Delsol et al. (16) reported seven cases of large B-cell lymphomas that express full-length ALK but are lacking the 2;5 translocation. These ALK-positive B-cell lymphomas express epithelial membrane antigen, CD4, CD57, and cytoplasmic IgA, but are negative for CD30, CD56 and other T- and B-cell markers. We present here a case resembling the ALK-positive large B-cell lymphoma proposed by Delsol et al. (16). Chromosomal and genomic analyses revealed that the lymphoma contains ALK fused to clathrin heavy chain gene (CLTC). We believe that our present observation is relevant for further understanding of the molecular mechanism underlying the development of this rare type of the lymphoma.
CASE REPORT
A 36-year-old Japanese female was admitted because of lumbago and constitutional symptoms. She had no specific individual or family history. Physical examination and laboratory tests on admission showed anemia (hemoglobin, 7.5 g/dL), mild hepatosplenomegaly, and IgG λ-type monoclonal gammopathy (IgG, 2782 mg/dL). Radiological studies showed multiple intramusucular tumors, bilateral ovarian tumors (right 70 × 48 mm, left 40 × 30 mm) and hepatosplenomegaly with no lymph node swellings. Although bone marrow aspiration was unsuccessful because of dry tap, a few blastic cells were observed. No sufficient diagnostic materials were obtained by bone marrow biopsy and needle biopsy of the intramuscular tumor. Finally, open biopsy of the left ovarian tumor was performed, which established the diagnosis of malignant lymphoma. Despite the treatment with combination chemotherapy, the lymphoma was primarily chemotherapy resistant, and the patient died 11 months after admission.
MATERIALS AND METHODS
Histopathology and Phenotyping
The tissue specimen was fixed in 10% formaldehyde and embedded in paraffin. Sections of 2–4 μm thickness were stained with hematoxylin and eosin. The avidin-biotin-peroxidase complex method was used for all immunohistochemical studies (epithelial membrane antigen, polyclonal CD3, L26 [CD20], mb-1 [CD79a], ALK1, Ber-H2 [CD30], anti-IgG, anti-κ, and anti-λ: DAKO, Copenhagen, Denmark; MT1 [CD43]: Bioscience, Emmerbruecke, Switzerland; 123C3 [CD56]: Zymed Laboratories, South San Francisco, CA; and UCHL-1 [CD45RO]: Nichirei, Tokyo, Japan).
Fresh specimens were also fixed in periodate-lysine-paraformaldehyde fixative, frozen, cut with a cryostat to a 6- to 8-μm thickness, fixed with acetone, and reacted with the primary antibodies (Leu1 [CD5], Leu2 [CD8], Leu3 [CD4], Leu5b [CD2], Leu7 [CD57], and Leu9 [CD7]: Becton Dickinson, Mountain View, CA; OKB22 [CD22] and OKT10 [CD38]: Ortho Diagnostic, Raritan, NJ; B4 [CD19]: Coulter Immunology, Hialeah, FL; and B-B4 [CD138]: Japan Tanner, Osaka, Japan). Sections were processed for avidin-biotin-peroxidase complex method.
Southern Blotting
High-molecular weight DNA was prepared by the conventional proteinase K digestion and phenol-chloroform extraction method. Ten micrograms of DNA was digested with appropriate restriction enzymes, subjected to electrophoresis on a 0.7% agarose gel, transferred to charged nylon membranes, and hybridized with human Ig or TCR gene probes labeled by random hexamer method.
In Situ Hybridization for Epstein-Barr Virus–Encoded RNA
In situ hybridization was performed as described previously (17). Briefly, after deparaffinization and digestion with proteinase K, the tissue sections were hybridized with fluorescein-conjugated oligonucleotide probes for Epstein-Barr virus–encoded RNA (Epstein-Barr virus probe in situ hybridization kit; Novocastra, Newcastle, England). Stringently washed sections were reacted with anti-fluorescein antibody and visualized with 5-bromo-4-chloroindolylphosphate and nitroblue tetrazolium salt.
Cytogenetics and Fluorescence In Situ Hybridization
Chromosomal analyses were performed by conventional G-banding and spectral karyotyping. Fluorescence in situ hybridization studies using 2p23 (ALK) breakpoint spanning and flanking probes (Vysis Inc., Downers Grove, IL) were performed on metaphase preparations according to the manufacturer’s instruction.
Reverse Transcription PCR and Sequencing
Five micrograms of total RNA extracted from frozen tissue was reverse-transcribed with Superscript II (Life Technologies, Rockville, MD). RT-PCR was performed as described by Bridge et al. (18) with CLTC-FWD primer (5′-TTAGATGCTTCAGAATCAC TG) and ALK-specific reverse primer (5′-TTCAGGC AGCGTCTTCACAG). The amplified fragments were cloned into plasmid vector using pGEM-T easy vector system (Promega, Madison, WI). Sequencing reaction was performed with BigDye terminator cycle sequencing kit (Applied Biosystems, Foster City, CA), and the reaction products were analyzed with ABI PRISM 310 Genetic analyzer.
RESULTS
Biopsy specimen obtained from the ovary showed monomorphic proliferation of large blastic cells with basophilic cytoplasm, round-shaped nuclei with high nuclear to cytoplasmic ratio, and prominent single nucleolus (Fig. 1A). Immunostaining with anti-ALK antibody showed finely granular cytoplasmic staining (Fig. 1B). This staining pattern was completely different from that of NPM-ALK fusion protein that was reported to be cytoplasm- and nuclear-associated (16). The tumor cells were positive for epithelial membrane antigen (Fig. 1C), CD4, CD19, CD38, and CD138, but negative for CD30 (Fig. 1D). Although these cells were negative for most of the other T-cell (CD2, CD3, CD5, CD7, CD8, CD43, CD45RO), B-cell (CD20, CD22, CD79a), and NK-cell (CD56, CD57) markers, the cytoplasm was strongly positive for IgG and λ chain (Fig. 1E). Southern blotting using Ig JH, Cλ, Cκ, and TCR Cβ1 probes showed the rearrangement of Cλ (Fig. 1F) and JH genes but not TCRβ gene, indicating B-cell origin of the neoplastic cells. Epstein-Barr virus–encoded RNA was not detected by in situ hybridization in these cells.

Characterization of the lymphoma cells. A–E, hematoxylin and eosin staining (A) and immunostaining for ALK (ALK1; B), epithelial membrane antigen (C), CD30 (Ber-H2; D), and λ chain (E; original magnification: A, B: 400 ×, C–E: 200 ×). F, Southern blot analysis with Ig Cλ probe. Ten-micrograms DNA digested by EcoRI + HindIII was electrophoresed, transferred to a nylon membrane, and detected by a probe corresponding to the Ig Cλ2 gene. Arrow indicates a rearranged band. Left lane: negative control (peripheral blood mononuclear cells obtained from a normal volunteer); right lane: lymphoma cells obtained from the left ovary.
Karyotypic analyses with G banding and spectral karyotyping techniques showed complex abnormality in which chromosome 2 was translocated to chromosome 17 (data not shown). Furthermore, fluorescence in situ hybridization analyses using ALK breakpoint probes showed a split of the two-color signals (data not shown), indicating a disruption of the 2p23 breakpoint. As a previous report of inflammatory myofibroblastic tumor (IMT) with t(2;17)(p23;q23) contained CLTC-ALK fusion transcript (18), we assumed that it might be also the case in the present patient. Reverse transcription PCR to detect the CLTC-ALK fusion transcript was performed, which amplified a 357-bp fragment (Fig. 2A). The sequence of the fragment was completely identical with that of the CLTC-ALK recognized in IMT cases (18; Fig. 2B).

Analyses of the CLTC-ALK fusion transcript. A, RT-PCR of the lymphoma cells. Lane 1, 1 kb plus DNA marker; Lane 2, negative control (PCR product without reverse transcriptase); Lane 3, RT-PCR product. B, sequence of the RT-PCR product.
DISCUSSION
Lymphoma cells in the present patient showed some unique properties: (1) cytoplasmic granular staining with anti-ALK antibody, (2) CD30−, epithelial membrane antigen+, CD4+, CD19+, CD20−, CD38+, CD138+, and cytoplasmic Ig+ phenotype and (3) Ig gene rearrangement. Most of these characteristics are consistent with those of ALK+, CD30−, CD20− large B-cell lymphoma originally reported by Delsol et al. (16). To the best of our knowledge, there has been thereafter only one similar case in the literature, as was reported by Gascoyne et al. (Table 2, Case 5 in Ref. 8). However, precise clinical and immunohistochemical records were lacking because this case was documented in a large series of ALCL. We thus consider that our present observation confirms the existence of ALK+, CD30−, CD20− large B-cell lymphomas proposed by Delsol et al. (16).
It is noteworthy that Delsol et al. (16) argued the expression of full-length ALK in this type of B-cell lymphomas. On the contrary, in the present patient, expression of CLTC-ALK fusion message, which is identical with that previously reported in ALCL (15) and IMT (18), was demonstrated. Interestingly, in a case of ALK-positive B-cell lymphoma shown by Gascoyne et al. (8), the 2;5 translocation was observed. Although the diversity of the fusion partner of the ALK gene in ALK-positive large B-cell lymphomas is entirely unclear, we speculate that ALK activation by itself is relevant irrespective of the fusion partner, as has been demonstrated in ALCL. It is also unclear why the identical translocation between ALK and CLTC can be found in different malignancies such as ALK+ large B-cell lymphoma, ALK+ ALCL of T/null-lineage, and IMT. One possible explanation for this phenomenon is that the translocation is a secondary event in the process of oncogenesis. Otherwise, the translocation may have occurred in a very primitive stage of the cellular differentiation such as in mesenchymal stem cells.
One of the interesting clinical features of the present patient was the association of monoclonal gammopathy. Previously, Delsol et al. (16) reported that ALK-positive large B-cell lymphomas show CD20−, CD19−, and VS38+ phenotype, suggesting their plasma cell origin. We consider that the association of monoclonal gammopathy, as well as CD38+, CD138+, CD19+, and CD20− phenotype, in the present patient supports their interpretation. We should also emphasize that the lymphoma cells in the present patient were found exclusively in extranodal sites such as bone marrow, liver, spleen, ovary, and muscle. Multiple intramuscular involvements are unusual among various types of lymphomas. Clinical and genetic data of more similar cases should be accumulated to further clarify the etiology, clinical features, and prognosis of the ALK+, CD30−, CD20− large B-cell lymphomas. In particular, it is mandatory to demonstrate the validity of discriminating the ALK-positive B-cell lymphomas from the classical diffuse large B-cell lymphomas.
References
Bitter MA, Franklin WA, Larson RA, McKeithan TW, Rubin CM, Le Beau MM, et al. Morphology in Ki-1 (CD30)-positive non-Hodgkin’s lymphoma is correlated with clinical features and the presence of a unique chromosomal abnormality, t(2;5)(p23;q35). Am J Surg Pathol 1990; 14: 305–306.
Lamant L, Meggetto F, al Saati T, Brugieres L, de Paillerets BB, Dastugue N, et al. High incidence of the t(2;5)(p23;q35) translocation in anaplastic large cell lymphoma and its lack of detection in Hodgkin’s disease. Comparison of cytogenetic analysis, reverse transcriptase-polymerase chain reaction, and P-80 immunostaining. Blood 1996; 87: 284–291.
Mason DY, Bastard C, Rimokh R, Dastugue N, Huret JL, Kristoffersson U, et al. CD30-positive large cell lymphomas (Ki-1 lymphoma) are associated with a chromosomal translocation involving 5q35. Br J Haematol 1990; 74: 161–168.
Wellmann A, Otsuki T, Vogelbruch M, Clark HM, Jaffe ES, Raffeld M . Analysis of the t(2;5)(p23;q35) translocation by reverse transcription-polymerase chain reaction in CD30+ anaplastic large-cell lymphomas, in other non-Hodgkin’s lymphomas of T-cell phenotype, and in Hodgkin’s disease. Blood 1995; 86: 2321–2328.
Morris SW, Kirstein MN, Valentine MB, Dittmer KG, Shapiro DN, Saltman DL, et al. Fusion of a kinase gene, ALK, to a nucleolar protein gene, NPM, in non-Hodgkin’s lymphoma. Science 1994; 263: 1281–1284.
Shiota M, Nakamura S, Ichinohasama R, Abe M, Akagi T, Takeshita M, et al. Anaplastic large cell lymphomas expressing the novel chimeric protein p80NPM/ALK: a distinct clinicopathologic entity. Blood 1995; 86: 1954–1960.
Nakamura S, Shiota M, Nakagawa A, Yatabe Y, Kojima M, Motoori T, et al. Anaplastic large cell lymphoma: a distinct molecular pathologic entity: a reappraisal with special reference to p80 (NPM/ALK) expression. Am J Surg Pathol 1997; 21: 1420–1432.
Gascoyne RD, Aoun P, Wu D, Chhanabhai M, Skinnider BF, Greiner TC, et al. Prognostic significance of anaplastic lymphoma kinase (ALK) protein expression in adults with anaplastic large cell lymphoma. Blood 1999; 93: 3913–3921.
Fujimoto J, Shiota M, Iwahara T, Seki N, Satoh H, Mori S, et al. Characterization of the transforming activity of p80, a hyperphosphorylated protein in a Ki-1 lymphoma cell line with chromosomal translocation t(2;5). Proc Natl Acad Sci U S A 1996; 93: 4181–4186.
Shiota M, Fujimoto J, Semba T, Satoh H, Yamamoto T, Mori S . Hyperphosphorylation of a novel 80 kDa protein-tyrosine kinase similar to Ltk in a human Ki-1 lymphoma cell line, AMS3. Oncogene 1994; 9: 1567–1574.
Bischof D, Pulford K, Mason DY, Morris SW . Role of the nucleophosmin (NPM) portion of the non-Hodgkin’s lymphoma-associated NPM-anaplastic lymphoma kinase fusion protein in oncogenesis. Mol Cell Biol 1997; 17: 2312–2325.
Stein H, Foss HD, Durkop H, Marafioti T, Delsol G, Pulford K, et al. CD30(+) anaplastic large cell lymphoma: a review of its histopathologic, genetic, and clinical features. Blood 2000; 96: 3681–3695.
Drexler HG, Gignac SM, von Wasielewski R, Werner M, Dirks WG . Pathobiology of NPM-ALK and variant fusion genes in anaplastic large cell lymphoma and other lymphomas. Leukemia 2000; 14: 1533–1559.
Morris SW, Xue L, Ma Z, Kinney MC . Alk+ CD30+ lymphomas: a distinct molecular genetic subtype of non-Hodgkin’s lymphoma. Br J Haematol 2001; 113: 275–295.
Touriol C, Greenland C, Lamant L, Pulford K, Bernard F, Rousset T, et al. Further demonstration of the diversity of chromosomal changes involving 2p23 in ALK-positive lymphoma: 2 cases expressing ALK kinase fused to CLTCL (clathrin chain polypeptide-like). Blood 2000; 95: 3204–3207.
Delsol G, Lamant L, Mariame B, Pulford K, Dastugue N, Brousset P, et al. A new subtype of large B-cell lymphoma expressing the ALK kinase and lacking the 2; 5 translocation. Blood 1997; 89: 1483–1490.
Chang JKC, Chen Y, Shibata D, Weiss L . Description of an in situ Epstein-Barr virus RNA in paraffin-embedded tissues, with a survey of normal and neoplastic tissues. Diagn Mol Pathol 1990; 1: 246–255.
Bridge JA, Kanamori M, Ma Z, Pickering D, Hill DA, Lydiatt W, et al. Fusion of the ALK gene to the clathrin heavy chain gene, CLTC, in inflammatory myofibroblastic tumor. Am J Pathol 2001; 159: 411–415.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Chikatsu, N., Kojima, H., Suzukawa, K. et al. ALK+, CD30−, CD20− Large B-Cell Lymphoma Containing Anaplastic Lymphoma Kinase (ALK) Fused to Clathrin Heavy Chain Gene (CLTC). Mod Pathol 16, 828–832 (2003). https://doi.org/10.1097/01.MP.0000081729.40230.1F
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1097/01.MP.0000081729.40230.1F
Keywords
This article is cited by
-
Diagnosis and treatment of CD20 negative B cell lymphomas
Biomarker Research (2017)
-
ALK-positive large B-cell lymphomas express a terminal B-cell differentiation program and activated STAT3 but lack MYC rearrangements
Modern Pathology (2013)
-
Anaplastic lymphoma kinase-positive diffuse large B cell lymphoma: immunohistochemical and FISH analysis of a rare tumor with unusual clinical presentation
Journal of Hematopathology (2013)
-
The clathrin-binding domain of CALM-AF10 alters the phenotype of myeloid neoplasms in mice
Oncogene (2012)
-
CD4-positive diffuse large B cell lymphoma identified by flow cytometry: two case reports
International Journal of Hematology (2010)
