
Abstract
Gliomas are the most frequent primary tumors of the central nervous system in adults. The most prevalent and aggressive subclass of these is glioblastoma multiforme, which is characterized by massive neovascularization. Endosialin (CD248) has generated interest as a target for antiangiogenic therapy following reports that its expression is upregulated on angiogenic endothelial cells. We demonstrate here that endosialin is not expressed in normal human adult brain but is strongly upregulated in the angiogenic vasculature of all high-grade glioma specimens examined. However, by taking advantage of a technique which allows for multiple fluorescent labeling of formalin-fixed paraffin-embedded archival sections, we demonstrate unambiguously that endosialin is not expressed by the glioma endothelial cells but on closely associated perivascular cells. With increasing awareness that targeting pericytes is an attractive adjunct in antiangiogenic therapy, this finding has important implications for understanding the molecular mechanisms regulating angiogenesis in these highly vascularized tumors.
Similar content being viewed by others


Main
Brain tumors account for approximately 20 500 new cases and 13 000 deaths each year in the United States.1 The most frequent primary brain tumors in adults are the gliomas, which represent a morphologically diverse set of malignancies diagnosed on the basis of their histology. These include diffuse astrocytomas (WHO grade II), anaplastic astrocytomas (WHO grade III) and glioblastomas (WHO grade IV).2 Glioblastoma multiforme is the most prevalent and aggressive type of glioma with a median survival of 12–15 months.3 Since standard therapy, especially in recurrent glioblastoma multiforme, has only limited impact on the survival of patients,4 a better understanding of the molecular alterations is needed to develop targeted treatment. Glioblastoma multiforme is considered an attractive target for antiangiogenic therapy, because one of its main characteristics is an extensive microvasculature, in some cases leading to multilayered glomeruloid-type microvascular proliferations.
Endosialin (CD248) raised interest as a potential therapeutic antiangiogenic target after it was identified in a SAGE screen as the most highly upregulated transcript in endothelial cells isolated from colon carcinomas compared to endothelial cells isolated from neighboring normal tissue, hence its alternate name of tumor endothelial marker 1 or TEM1.5 Endosialin is a type 1 transmembrane glycoprotein originally identified as the target of the FB5 monoclonal antibody.6 The domain structure of endosialin, with a C-type lectin-like domain, a sushi domain, three epidermal growth factor repeats and a serine/threonine rich mucin-like stalk has placed it in a family of proteins together with CD93 (the complement receptor C1qRp) and CD141 (thrombomodulin).7 In cultured cells, expression of endosialin has only been reported on fibroblasts and some neuroblastoma cell lines.6, 7, 8, 9 This pattern is reflected in normal adult tissue, where endosialin expression is predominantly restricted to stromal fibroblasts, and in agreement with the SAGE analysis of St Croix et al5 little or no endosialin is detected in the mature, normal vasculature.9, 10, 11, 12, 13 In contrast, there is a marked upregulation of endosialin expression in the angiogenic vasculature of a wide variety of different tumor types including those of the brain, colon, breast and in tumor xenografts.6, 9, 11, 12, 14, 15 However, there is controversy between these reports as to whether this upregulation is due to expression by the endothelial cells and/or the perivascular cells. Two major difficulties have arisen in resolving this controversy. First, double labeling studies have traditionally required the staining of cryosections, in which the cell and tissue morphology are less well preserved. In addition, the availability of fresh tumor material required for cryosections is very limited in comparison to the large collections of formalin-fixed paraffin-embedded tissues. Second, the close proximity of stromal fibroblasts near the angiogenic vasculature has resulted in some debate as to whether expression of endosialin on cells adjacent to angiogenic endothelial cells represents expression on pericytes or closely associated fibroblasts.
To specifically address both these issues, we have examined the expression of endosialin in a series of high-grade gliomas. The benefits of using brain tissue are the low number of stromal fibroblasts and the presence of an extensive vasculature. In addition, we have employed an immunofluorescent labeling technique, which allows high-resolution multicolor imaging of formalin-fixed paraffin-embedded sections. Together this has allowed us to demonstrate unambiguously that expression of endosialin in the angiogenic vasculature of high-grade gliomas is restricted to perivascular cells, and that endosialin is not detected on the endothelial cells.
Materials and methods
Samples
Brain tumor samples were obtained after approval by Local and Multicentre Ethical Review Committees from the Royal Marsden Hospital, Sutton, and St Georges Hospital Medical School, London, UK. In total, 10 high-grade gliomas were studied, comprising eight WHO grade IV glioblastoma multiforme, and two grade III anaplastic astrocytoma. The age range was from 31–72 years. Paraffin-embedded normal adult brain from individuals with no history of neurological disease was provided by Dr Peter Clark, Imperial College London from the UK Multiple Sclerosis Tissue Bank, Imperial College London, and was processed using standard histological techniques.16
Antibodies and Cells
The generation of the human anti-endosialin monoclonal antibodies (B1/35 and B1/22) has been described previously.9 The following antibodies were obtained commercially: anti-α-tubulin (clone: B-5-1-2, Sigma-Aldrich, St Louis, MO, USA), anti-human-α-smooth muscle actin (clone: 1A4, Sigma-Aldrich), anti-human-CD34 monoclonal antibody (clone: QBEND 10, Sky Bio, Bedfordshire, UK), fluorescein isothiocyanate-conjugated anti-human CD34 monoclonal antibody (clone: QBEND 10, Abcam, Cambridge, UK), Horseradish peroxidase (HRP)-anti-mouse Ig (Jackson Immunoresearch, West Grove, PA, USA), Alexa-conjugated second layer antibodies (Molecular Probes, Eugene, OR, USA). Diploid human AG1523 fibroblasts and human MCF7 epithelial breast carcinoma cells were cultured in Dulbecco's modified Eagle's medium supplemented with 10% fetal bovine serum, 2 mM L-glutamine and penicillin/streptomycin. Human MCF10A mammary epithelial cells were grown in Dulbecco's modified Eagle's medium:F12, supplemented with 5% horse serum, 10 μM HEPES, 10 μg/ml insulin, 20 ng/ml EGF, 0.5 μg/ml hydrocortisone, 100 ng/ml cholera toxin. Cells were cultured at 37°C in a tissue culture incubator with humidified air, supplemented with CO2 to 10%.
Western Blot Analysis
Cells were lysed in NuPage non-reducing sample buffer and run on 10% SDS-PAGE gels. Gels were transferred onto nitrocellulose membrane, blocked with 5% low-fat milk and incubated with the primary antibodies: B1/35, B1/22 (0.2 μg/ml) and α-tubulin (1:30 000 dilution), followed by horseradish peroxidase-conjugated anti-mouse IgG (0.2 μg/ml). Immunodetection was carried out using the ECL Kit (Amersham, Buckhinghamshire, UK) followed by exposure to X-ray film (Kodak, Rochester, NY, USA) for 20 min.
Immunohistochemistry
Formalin-fixed paraffin-embedded sections (3 or 4 μm) were dewaxed in xylene (2 × 5 min) and rehydrated through a series of graded alcohols to water. Slides were then pressure cooked for 2 min in 0.01 M pH 6.0 citrate target retrieval buffer, washed 5 min under running water and stained with the anti-endosialin monoclonal antibodies (B1/35, B1/22, 2 μg/ml) or with anti-CD34 monoclonal antibodies at a 1:50 dilution for 1 h at room temperature. Detection was achieved with the Vectastain avidin–biotin complex (ABC) system according to the manufacturer's protocol (Vector Laboratories, Burlingame, CA, USA). Finally slides were dehydrated through a series of alcohols, cleared in xylene and mounted in 1,3-diethyl-8-phenylxanthine. Sections of human placenta served as positive control for stainings. Images were captured on a Leica DMRA2 microscope fitted with a Leica DFC320 camera and processed with Adobe Photoshop 7.0. All images were taken at the same camera settings.
Confocal Microscopy
Staining of cells on glass coverslips was performed as described previously.13 For confocal microscopy of formalin-fixed paraffin-embedded material, sections were dewaxed and rehydrated and then antigen retrieval was performed at 95°C in DAKO Cytomation target retrieval solution (DAKO, Denmark) for 30 min followed by 20 min at room temperature and 5 min under running water. Slides were removed from water, sections marked using a slide marker pen and incubated with primary antibodies for 1 h at room temperature. After 3 × 5 min wash with PBS the appropriate secondary antibodies were incubated for 1 h at room temperature. For double labeling of endosialin and CD34, staining was performed in the following order: B1/35 (2 μg/ml), Alexa555 anti-mouse Ig (2 μg/ml), FITC-conjugated CD34 monoclonal antibody (2.5 μg/ml). For double labeling of endosialin and α-smooth muscle actin, slides were incubated with B1/35 (2 μg/ml) and anti-α-smooth muscle actin (0.88 μg/ml) followed by the 2 μg/ml Alexa555-conjugated anti-mouse-IgG1 (to detect monoclonal antibody B1/35) and 2 μg/ml Alexa488-anti-mouse-IgG2A (to detect the anti-α-smooth muscle actin monoclonal antibody). Control experiments showed that there was no non-specific binding or cross-reactivity of the secondary antibodies. Nuclei were counterstained with 14 nM DAPI (Molecular Probes), slides were rinsed in PBS, mounted with Vectashield (Vector Laboratories) and the coverslips sealed with nail varnish. Fluorescent images were collected sequentially in three channels on a Leica Microsystems (Leica, Wetzlar, Germany) TCS-SP2 confocal microscope. All images were taken at the same settings. Images were exported from the Leica software and processed with Adobe Photoshop 7.0. A full method describing the immunofluorescent staining of formalin-fixed paraffin-embedded sections has been submitted for publication (Robertson D, Savage K, Reis-Filho JS and Isacke CM).
Results
Characterization of the Human Endosialin Monoclonal Antibodies
We have previously described four monoclonal antibodies which recognize human endosialin in immunoprecipitation and immunofluorescence experiments.9 Here, we have further characterized two of these anti-endosialin monoclonal antibodies, B1/35 and B1/22 by immunoblotting and immunofluorescent staining. Western blots on lysates of AG1523 human fibroblasts, which endogenously express endosialin, demonstrated that both monoclonal antibodies recognize the mature 175 kDa protein and a lower 80 kDa molecular weight band (Figure 1a). This banding pattern has been reported previously for both human and mouse endosialin detected with other monoclonal antibodies and polyclonal antibodies.7, 8, 12, 13 The 80 kDa band most likely represents a population of intracellular immaturely glycosylated endosialin as both these monoclonal antibodies have previously been shown to only recognize the 175 kDa endosialin following immunoprecipitation of cell surface labeled human fibroblasts.9 Neither monoclonal antibody demonstrated any reactivity with lysates from endosialin-negative MCF7 cells (Figure 1a). In immunofluorescent staining of cells in culture, B1/35 and B1/22 showed an identical granular distribution of endosialin on the plasma membrane of AG1523 fibroblasts but showed no staining of MCF10A epithelial cells (Figure 1b). Finally to assess the ability of these monoclonal antibodies to recognize endosialin in formalin-fixed paraffin-embedded material, sections of normal human breast were stained. As shown in Figure 1c, both antibodies were able to detect endosialin on the interlobular and intralobular fibroblasts but not on either the myoepithelial or luminal epithelial cells. This expression is identical to that previously reported following staining of endosialin on normal breast cryosections.9 As no differences in reactivity in any of these assays were observed between the independently isolated B1/35 and B1/22 anti-endosialin monoclonal antibodies, only B1/35 was used for further experiments.

Characterization of the human endosialin monoclonal antibodies. (a) Lysates of AG1523 human fibroblasts (F) and MCF7 human epithelial cells (E) were subject to immunoblotting using either monoclonal antibody B1/35, monoclonal antibody B1/22 or an anti-α-tubulin (tub) monoclonal antibody as a loading control. (b) AG1523 fibroblasts (F) and MCF10A epithelial cells (E) were fixed in 4% paraformaldehyde, permeabilized with 0.5% Triton X-100 and stained with the monoclonal antibodies B1/35 or B1/22 followed by Alexa488-anti-mouse IgG (green) and counterstained with TO-PRO-3 (blue). Scale bar, 50 μm. (c) Formalin-fixed paraffin-embedded sections of normal breast were stained with the monoclonal antibody B1/35 or B1/22 and counterstained with haematoxylin. Arrows indicate endosialin-expressing fibroblasts. Arrowheads indicate endosialin-negative epithelial cells. Scale bar, 150 μm.
Endosialin Expression is Upregulated on the Vasculature of High-Grade Gliomas
To assess expression of endosialin in normal adult human brain and high-grade gliomas, formalin-fixed paraffin-embedded sections were stained with the anti-endosialin monoclonal antibody B1/35 and parallel sections were stained for the endothelial marker CD34. In normal brain, the vasculature was detected with the anti-CD34 monoclonal antibody but no staining was observed on the vasculature or on any other cell types with B1/35 (Figure 2a). In contrast, endosialin expression was readily detected in the vasculature of 10 different high-grade gliomas, with stronger staining observed in the 8 grade IV gliomas compared to the 2 grade III anaplastic astrocytomas (Table 1, Figure 2b). In the higher grade tumors, endosialin expression was detected on the small vessels and the glomeruloid microvascular proliferations.

Histopathological assessment of endosialin expression in normal adult human brain and high-grade gliomas. Formalin-fixed paraffin-embedded sections were stained with haematoxylin and eosin (H&E), the anti-endosialin monoclonal antibody B1/35 or with anti-CD34 monoclonal antibody. (a) Temporal lobe (Temp) and cerebellum (CBM) of normal adult human brain. Arrows indicate endosialin-negative vessels. Scale bar, 150 μm. (b) Representative images from 1 grade III tumor (3314) and 3 grade IV tumors (3455, 3384, and 3358). Arrows indicate endosialin-positive vessels. Arrowheads indicate strongly stained glomeruloid microvascular proliferations. Results from all 10 high-grade glioblastomas are summarized in Table 1. Scale bar, 150 μm.
Endosialin is Expressed by Pericytes in High-Grade Gliomas but not by Endothelial Cells
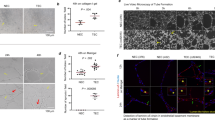
To better assess the cell type distribution of endosialin in the tumor vasculature, formalin-fixed paraffin-embedded sections were double labeled for endosialin and markers of either endothelial or perivascular cells and images were collected by confocal microscopy. Using this high resolution imaging method, it was clearly demonstrated that there was no overlap in staining of endosialin and the endothelial marker CD34 (Figure 3a). To verify the location of endosialin on cells adjacent to the endothelium, sections were costained with the pericyte marker, α-smooth muscle actin. As illustrated in Figure 3b, the majority of endosialin-positive cells also stained positive for α-smooth muscle actin and in addition, a small number of dispersed endosialin-positive, α-smooth muscle actin-negative stromal fibroblasts were also identified.

Distribution of endosialin on tumor-associated vessels in high-grade gliomas. Formalin-fixed paraffin-embedded sections of grade IV gliomas were costained with (a) monoclonal antibody B1/35 (red) and anti-CD34 (green) or (b) monoclonal antibody B1/35 (red) and anti-α-smooth muscle actin (green). Nuclei were counterstained with DAPI (blue). Arrowheads indicate endothelial cells. Arrows indicate perivascular cells. *Indicates endosialin-positive, α-smooth muscle actin-negative fibroblasts. Scale bar, 50 μm in main panels and 20 μm in merge × 2.5 panels.
Discussion
To date there has been a controversy in the literature as to the cell type expression of endosialin in the tumor vasculature. Endosialin was first identified as the epitope for monoclonal antibody FB56 and staining with this antibody revealed an upregulation of endosialin expression in the vasculature of a variety of human tumors. Despite reporting that this represented expression on the endothelial cells, the cell type distribution was not validated by double labeling with endothelial markers. Similarly, in situ hybridization analysis has demonstrated an upregulation of endosialin mRNAs in the tumor vasculature but again this method cannot distinguish between an endothelial and perivascular localization of the signal.5, 14, 17 As endosialin is also expressed in the developing vasculature, different laboratories have performed double labeling of cryosections both from tumors and developing tissues. However, disparate results have been obtained in that it has been reported that endosialin is only expressed on the endothelial cells,12 only on the pericytes9, 13, 18 and on both.15 The main problem in such analysis is that in tissue cryosections it can be difficult to distinguish between an overlapping staining pattern and staining of individual cells which are intimately associated, as is the case for endothelial cells and pericytes.
To address this controversy, we first characterized further two anti-endosialin monoclonal antibodies, B1/35 and B1/22. Both antibodies showed an identical cell surface staining and western blotting pattern on cultured human fibroblasts and importantly both antibodies were able to detect endosialin in formalin-fixed paraffin-embedded sections. Monoclonal antibody B1/35 was then used to characterize the expression of endosialin in normal brain and in high-grade gliomas. In agreement with previous studies in the mouse brain and human brain tumor samples,12, 13, 15 no expression of endosialin was detected in the normal adult human brain but expression was upregulated in the vasculature of all high-grade gliomas examined. Highest levels of expression were found in the grade IV gliomas and in particular on the glomeruloid microvascular proliferations. These are tufted collections of newly formed vascular channels containing hyperplastic endothelial cells surrounded by numerous pericytes and a basal lamina.19 Next, we combined immunofluorescent double labeling of formalin-fixed paraffin-embedded sections with high resolution confocal imaging of thin (∼0.5 μm) optical sections. Costaining of these sections with the anti-endosialin monoclonal antibody B1/35 and with an antibody against the endothelium-specific marker CD34 revealed a clear separation of the two antibodies, with the endosialin-positive cells lying adjacent to the endothelial cells. This separation of staining was detected in both the smaller vessels and the larger complex glomeruloid microvascular proliferations. Double labeling of sections with antibodies against endosialin and the frequently used pericyte marker α-smooth muscle actin,20, 21, 22 confirmed that endosialin is expressed by α-smooth muscle actin-positive pericytes.
In conclusion, endosialin is not expressed in the vasculature of normal adult brain but strongly upregulated in tumor vessels in high-grade gliomas. By employing confocal microscopy of immunolabeled formalin-fixed paraffin-embedded sections, it was unambiguously shown that the expression of endosialin is restricted to perivascular cells and some scattered fibroblasts, validating endosialin as a robust pericyte marker. The significance of these findings is twofold. First, mice with a homozygous deletion in endosialin (Cd248) show impaired growth, invasion and vascularization of implanted abdominal tumors,17 suggesting that endosialin expression on pericytes has an important functional role in the tumor vasculature. Second, there is increasing evidence that antiangiogenic therapies targeting both endothelial cells and pericytes are more effective than single-agent therapies.23 Endosialin, unlike other pericyte makers, is not expressed in the normal vasculature, but strongly upregulated in the tumor vasculature. As a consequence targeting endosialin or pathways associated with this receptor offer an attractive therapeutic opportunity. This may be particularly relevant to glioblastoma multiforme, which is characterized by extensive microvascular proliferation, but for which there is currently little targeted treatments.
References
Jemal A, Siegel R, Ward E, et al. Cancer statistics, 2007. CA Cancer J Clin 2007;57:43–66.
Louis DN, Ohgaki H, Wiestler OD, et al. The 2007 WHO classification of tumours of the central nervous system. Acta Neuropathol (Berl) 2007;114:97–109.
Stupp R, Mason WP, van den Bent MJ, et al. Radiotherapy plus concomitant and adjuvant temozolomide for glioblastoma. N Engl J Med 2005;352:987–996.
Simpson L, Galanis E . Recurrent glioblastoma multiforme: advances in treatment and promising drug candidates. Expert Rev Anticancer Ther 2006;6:1593–1607.
St Croix B, Rago C, Velculescu V, et al. Genes expressed in human tumor endothelium. Science 2000;289:1197–1202.
Rettig WJ, Garin-Chesa P, Healey JH, et al. Identification of endosialin, a cell surface glycoprotein of vascular endothelial cells in human cancer. Proc Natl Acad Sci USA 1992;89:10832–10836.
Christian S, Ahorn H, Koehler A, et al. Molecular cloning and characterization of endosialin, a C-type lectin-like cell surface receptor of tumor endothelium. J Biol Chem 2001;276:7408–7414.
Opavsky R, Haviernik P, Jurkovicova D, et al. Molecular characterization of the mouse Tem1/endosialin gene regulated by cell density in vitro and expressed in normal tissues in vivo. J Biol Chem 2001;276:38795–38807.
MacFadyen JR, Haworth O, Roberston D, et al. Endosialin (TEM1, CD248) is a marker of stromal fibroblasts and is not selectively expressed on tumour endothelium. FEBS Lett 2005;579:2569–2575.
Dolznig H, Schweifer N, Puri C, et al. Characterization of cancer stroma markers: in silico analysis of an mRNA expression database for fibroblast activation protein and endosialin. Cancer Immun 2005;5:10.
Huber MA, Kraut N, Schweifer N, et al. Expression of stromal cell markers in distinct compartments of human skin cancers. J Cutan Pathol 2006;33:145–155.
Rupp C, Dolznig H, Puri C, et al. Mouse endosialin, a C-type lectin-like cell surface receptor: expression during embryonic development and induction in experimental cancer neoangiogenesis. Cancer Immun 2006;6:10.
MacFadyen J, Savage K, Wienke D, et al. Endosialin is expressed on stromal fibroblasts and CNS pericytes in mouse embryos and is downregulated during development. Gene Expr Patterns 2007;7:363–369.
Carson-Walter EB, Watkins DN, Nanda A, et al. Cell surface tumor endothelial markers are conserved in mice and humans. Cancer Res 2001;61:6649–6655.
Brady J, Neal J, Sadakar N, et al. Human endosialin (tumor endothelial marker 1) is abundantly expressed in highly malignant and invasive brain tumors. J Neuropathol Exp Neurol 2004;63:1274–1283.
Williams MJ, Lowrie MB, Bennett JP, et al. Cadherin-10 is a novel blood–brain barrier adhesion molecule in human and mouse. Brain Res 2005;1058:62–72.
Nanda A, Karim B, Peng Z, et al. Tumor endothelial marker 1 (Tem1) functions in the growth and progression of abdominal tumors. Proc Natl Acad Sci USA 2006;103:3351–3356.
Virgintino D, Girolamo F, Errede M, et al. An intimate interplay between precocious, migrating pericytes and endothelial cells governs human fetal brain angiogenesis. Angiogenesis 2007;10:35–45.
Kargiotis O, Rao JS, Kyritsis AP . Mechanisms of angiogenesis in gliomas. J Neurooncol 2006;78:281–293.
Haddad SF, Moore SA, Schelper RL, et al. Vascular smooth muscle hyperplasia underlies the formation of glomeruloid vascular structures of glioblastoma multiforme. J Neuropathol Exp Neurol 1992;51:488–492.
Wesseling P, Vandersteenhoven JJ, Downey BT, et al. Cellular components of microvascular proliferation in human glial and metastatic brain neoplasms. A light microscopic and immunohistochemical study of formalin-fixed, routinely processed material. Acta Neuropathol (Berl) 1993;85:508–514.
Wesseling P, Schlingemann RO, Rietveld FJ, et al. Early and extensive contribution of pericytes/vascular smooth muscle cells to microvascular proliferation in glioblastoma multiforme: an immuno-light and immuno-electron microscopic study. J Neuropathol Exp Neurol 1995;54:304–310.
Bergers G, Song S, Meyer-Morse N, et al. Benefits of targeting both pericytes and endothelial cells in the tumor vasculature with kinase inhibitors. J Clin Invest 2003;111:1287–1295.
Acknowledgements
We thank Dr Darren Hargrave (Royal Marsden Hospital) and Dr Peter Wilkins (St Georges Hospital Medical School) for providing the high-grade glioma samples and clinicopathological data, Peter Clark (Imperial College, London) for providing the normal brain samples, and Kay Savage and Suzanne Parry (Breakthrough Histopathology Laboratory, Institute of Cancer Research) for immunohistochemical staining of the sections. This work was funded by a grant from Breakthrough Breast Cancer (CMI) and Cancer Research UK (CJ).
Author information
Authors and Affiliations
Corresponding author
Additional information
Disclosure/duality of interest
There are no disclosures or duality of interests to declare.
Rights and permissions
About this article
Cite this article
Simonavicius, N., Robertson, D., Bax, D. et al. Endosialin (CD248) is a marker of tumor-associated pericytes in high-grade glioma. Mod Pathol 21, 308–315 (2008). https://doi.org/10.1038/modpathol.3801006
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/modpathol.3801006
Keywords
This article is cited by
-
Group XIV C-type lectins: emerging targets in tumor angiogenesis
Angiogenesis (2024)
-
Interference in melanoma CD248 function reduces vascular mimicry and metastasis
Journal of Biomedical Science (2022)
-
177Lu radiolabeling and preclinical theranostic study of 1C1m-Fc: an anti-TEM-1 scFv-Fc fusion protein in soft tissue sarcoma
EJNMMI Research (2020)
-
A phase I study of ontuxizumab, a humanized monoclonal antibody targeting endosialin, in Japanese patients with solid tumors
Investigational New Drugs (2019)
-
Blocking CD248 molecules in perivascular stromal cells of patients with systemic sclerosis strongly inhibits their differentiation toward myofibroblasts and proliferation: a new potential target for antifibrotic therapy
Arthritis Research & Therapy (2018)
