
Abstract
Study design:
Cross-sectional study.
Objectives:
(1) To examine whether the Klein–Bell ADL Scale (K–B Scale) discriminates cervical spinal cord injury (SCI) patients in daily activities and to explore its applicability in this group of patients. (2) To examine the association between basic ADL and upper extremity function. (3) To investigate if grip ability can be discerned in the scale.
Setting:
Spinal Cord Injury Unit, Sahlgrenska University Hospital, Göteborg, Sweden.
Methods:
Fifty-five patients with cervical SCI with no prior reconstructive hand surgery were included in the study. Analyses of the patient's independence were made according to the K–B Scale. Three additional analyses were carried out, the first examined whether the use of assistive devices and house and car adaptations influenced independence. The last two used different approaches to investigate whether arm and grip function could be detected in the K–B scale.
Results:
Raw score in the K–B Scale can discriminate for independence in daily activities but the scale's weight scheme does not function for cervical SCI patients. Assistive devices and car and house adaptations can compensate for dependence in daily activities. Lack of grip function decreases the patient's ability to become independent. Diagnosis-related activities cannot be assessed in all items.
Conclusion:
The K–B Scale's raw score was useful assessing daily activities in cervical SCI patients. Its reliability in conjunction with arm and grip function in patients with cervical SCI has yet to be proven.
Similar content being viewed by others


Introduction
A spinal cord injury (SCI) instantly changes a person's life forever.1 The consequences of the injury are reflected in the extent of loss of motor and sensory function and the resulting inability to perform activities of daily living (ADL).2 For an individual with a SCI affecting the cervical level even the most basic ADL tasks becomes a challenge. It can render the individual dependent upon assistance in many areas of daily living.1, 3 Important prerequisites for ADL are upper extremity function4, 5 and physical capacity.6 Other important factors are age, gender, body mass,7 physical fitness,7, 8 motivation, psychosocial status, medical complications8 and socio-cultural background.9 Earlier studies5, 10 have shown that preserved motor level can predict the ability of patients with cervical SCI to become independent in ADL. The International Classification of Functioning, Disability and Health (ICF) provides an interactive framework, wherein body functions and structures, activities and participation, environmental and personal components are related and influence one another.11 The ICF can be used as a reference for already existing outcome measurements to provide a clear picture of which health domains that are addressed by the different measurements.12
Reconstructive arm and hand surgery has the potential to improve both passive and active function in the arm and hand in patients with cervical SCI.13, 14 The basis for treatment is the patient's needs and desires as well as the remaining motor and sensory functions in the upper extremities, with no restrictions related to age or time since injury.15 Even though hand function is of the utmost importance for independence in ADL, the evaluation of reconstructive hand surgery has hitherto been focused more on assessing function than activity.16, 17 Today there are no generally accepted ways to measure the improvement of hand function and ADL in connection with reconstructive hand surgery.18 The diagnose-specific outcome measurement Quadriplegia index of Function (QIF)19 existed at the time of the study. However, the QIF's activities are not divided into parts and can therefore not be used to assess independence in daily activities in detail.
For this study, we were interested in an appropriate instrument with relevant components of activities that could discriminate the patient's levels of independence in carrying out basic ADL in connection with reconstructive hand surgery. The Klein–Bell ADL Scale (K–B Scale)20, 21 is a generic instrument that can be applied in persons with or without disability and is constructed to measure basic ADL in detail. The activities are divided into essential components (items) and each component is scored separately. Previous studies demonstrated reliability21, 22, 23 and validity21, 23 as well as sensitivity toward small changes in ADL.22, 24 However, in earlier studies the SCI patients level of injury either remain unclear21 or include few cervical SCI patients.25 It is therefore important to investigate if the K–B Scale is an appropriate instrument to measure basic ADL in patients with cervical SCI.
The aims of this study were to examine whether the K–B Scale as a generic instrument can discriminate between patients with cervical SCI and to explore the applicability of the scale among the same group. Furthermore, the purpose was to examine the association between basic ADL and upper extremity function and finally to investigate if grip ability can be discerned in the scale.
Methods
This study used a cross-sectional approach and is part of an ongoing intervention study. Only data preceding the intervention were used in the present paper. The patients were asked to participate in the study during their first visit to the Hand Team at the Spinal Cord Injury Unit (SCI Unit) at Sahlgrenska University Hospital, Göteborg, Sweden. The patients included in this study met the following criteria: (a) traumatic SCI or acute vascular injury in the cervical level of the spinal cord, (b) no prior reconstructive hand surgery before September 1994. The data were collected from September 1994 to November 2003 and no patient declined participation in the interviews preceding the arm/hand surgery in the study.
Patients
A total of 55 patients with cervical SCI were included in the study, 43 (78%) men and 12 (22%) women (mean age 39 years, range 18–72 years). The duration from the time of injury was 1–37 years (mean 5.5 years). Thirty-one patients lived together with partners, 18 were single and six lived together with their parents. Forty-nine patients used wheelchairs, four were ambulatory and two used wheelchairs part-time and were part-time ambulatory.
Test of motor function was measured with the manual muscle test (MMT) using Medical Research Council (MRC)26 grades from 0 to 5 in the upper extremities from the trapezius to the intrinsic muscles (20 muscles) according to Ejeskar.15 The maximum sum score for upper extremity motor score (UEMS)10 is 100 points in each arm, that is, 200 points for both arms together.26
The American Spinal Injury Association (ASIA)2 motor level and motor score was derived from the MMT test. The patient's motor level ranged from no motor function to full motor function (C4 to C8) in both the right and left arm and hand according to ASIA. The ASIA motor levels showed that 33 patients (60%) were found to have the same motor level in both arms, whereas 20 patients (36%) showed an asymmetric pattern. Two patients (2%) were not included due to lack of data in the MMT test (Table 1). The ASIA motor score ranged between 2 and 20 points in the right hand and between 0 and 20 points in the left hand (Figure 1).

The ASIA motor score from C5 to C8 in right arm and left arm (maximum of 20 points per arm) (n=53)
Sensory function was measured using two-point discrimination (2PD) on the palmar aspect of the distal phalanx of all fingers. The threshold ⩽10 mm is known to be a valid measure of useful finger proprioception and when present the hand can be used for afferent control of grip function according to Moberg.27 The 2PD values for the thumb, middle finger and little finger was translated to sensory level according to ASIA.2 As only C6, C7 and C8 dermatomes were used for sensory testing, it is not possible to give an accurate ASIA grading of the degree of injury.
Nine patients (16%) lacked sensation in all fingers in both right and left hand, 10 patients (18%) had remaining sensation on C6 level in one hand, 13 patients (24%) had sensory function on C6 level in both right and left hand, 13 patients (24%) had sensory function in both hands from C6 to C8 level and eight patients (15%) had full sensation in both hands. In two patients (2%), the 2PD test was not performed in one hand. The hand surgeons were responsible for the MMT test and the 2PD test. A specialist in neurology classified the patients according to the ASIA motor level and ASIA sensory level. The data were derived from the MMT test and the 2PD test.
Measurements
The K–B Scale20, 21 can measure patient's level of independence in basic ADL with a raw score or with a weight score in 170 items.20, 21 The items in the scale are divided into six dimensions: dressing, elimination, mobility, bathing and hygiene, eating and emergency telephone use.
The items in the K–B Scale were linked28 in the present study to the ICF to investigate which health domains were covered in the scale. The majority of items (162 items) measure ADL (dressing, bladder and bowel management, mobility, hygiene, eating and drinking and using the telephone), whereas eight items measure body function (bladder and bowel emptying, bladder and bowel incontinence, chewing and swallowing food, swallowing liquids, verbalizing telephone messages).
Klein and Bell20, 21 developed a weight scheme under the assumption that some items are more difficult, time consuming etc than others. Each item was rated in an empirical manner on a five-point scale with four criteria's: ‘1. How difficult is it for average able-bodied persons? 2. How difficult is it for the average able-bodied person to perform this activity for someone else (to provide maximum assistance)? 3. How much time does it take to perform this activity? 4. How injurious to one's health would it be if the activity could not be performed?’ (Klein and Bell,21 pp 336). A mean rating was obtain for each rater and frequency distribution was calculated for each item and the items were thereafter given a weight score from 1 to 3, where weight 3 is given to the most complex items.20, 21 The weights 1, 2 and 3 from the original construction will be used in the analysis. The weights will be referred to as simple, average complex and complex, respectively.20 Eleven items in the K–B Scale lack individual weight score in the weight scheme.20 For this reason, only 159 items were included in the analysis of the weight scheme. The 159 items in the weight scheme are divided into 29 simple items, 108 average complex items and 22 complex items.20, 21
The K–B scale has been translated into Swedish29 and was validated in three studies.30, 31, 32 In the present study, the assessment of patient's level of independence in basic ADL was made via a semistructured interview conducted by the first author. The K–B Scale was presented verbally to the patient before the interview. All interviews were conducted at the SCI Unit. The patients in this study were asked what they in fact do or carry out on a regular basis to assess the actual activity level in the person's real life surroundings. Diagnosis-specific questions were used to verify uncertain answers during the interview and to include more information, such as on the use of assistive devices and car and house adaptations. The dichotomized categories of independent with or without assistive devices (three points) and dependent with verbal or physical assistance (0 point)20, 21 in each item were used to analyze the patients' independence. Gender-specific items for the opposite gender and diagnose-specific items were registered as not applicable items.
A data program called the ADL diagram©33 was developed to compile the raw score to recommendations in the K–B Scale manual.20, 21, 34 The analyses made with the ADL diagram© show each item per patient and raw sum score in 170 items. A patient who carries out an item independently receives a raw score of three points; if he/she is unable to carry out the item, a raw score of zero points is given. The raw sum score in the K–B Scale range from 0 (dependence) to 510 points (independence).34
Statistical methods
Spearman's rank correlation test was used to statistically analyze raw sum score in the K–B Scale and UEMS in both arms for the patients in order to detect whether a relationship existed between independence in ADL and upper extremities function. Spearman's rank correlation test was also used to statistically analyze raw sum score in the K–B Scale and the sensory function in number of fingers with ⩽10 mm in the 2PD test to detect whether a relationship existed between independence in ADL and sensory function in the hands. The correlation coefficients is interpreted according to Munro35 as 0.00–0.25: little if any correlation; 0.26–0.49: low correlation; 0.50–0.69: moderate correlation; 0.70–0.89: high correlation; 0.90–1.00: very high correlation. Two patients were excluded owing to a lack of MMT scores and two patients were excluded owing to lack of 2PD tests, 53 patients were included in both tests.
A statistical analysis was performed to investigate if a difference of complexity existed between the original weight levels in the K–B Scale.20, 21 The original weight levels in the K–B Scale (simple, average complex, complex) were compared with paired T-test and 95% confidence intervals for the mean differences.36 For each patient the following differences were calculated; simple–average complex, average complex–complex and simple–complex levels. These differences were based on the patients' individual percent of raw sum score in each weight level. A value of P<0.05 (two-sided) was considered significant. Statistical analysis was carried out using statistical software (SPSS 13.0 for Windows®).
Three more analyses were performed and the results of these three analyses are given in descriptive statistics. The first analysis was made to examine whether the patients' use of assistive devices and house and car adaptations influenced their independence. In the second analysis, the K–B Scale was to linked28 the ICF11 to examine whether arm and grip function could be detected in the items' operational criteria. In the last analysis, Napier's37 definition of precision and power grips together with Bendz's38 description of grip ability from the opening phase to the terminal opening phase in the grip procedure was used to investigate whether these components could be detected in the items' operational criteria.
Results
Discrimination and applicability of the K–B ADL Scale
The patients' level of independence according to the raw sum score ranged from 42 to 456 points in the K–B Scale. Thirty-two of 55 patients had less than 50% of the raw sum score (Figure 2).

Level of independence with raw sum score in basic activities of daily living among patients with cervical SCI according to the Klein–Bell ADL Scale. (n=55)
In Figure 3, 159 items in the dimensions (emergency telephone use, eating, mobility, hygiene and bathing, dressing, and elimination) according to the K–B Scale are ordered with respect to the proportion of independent patients from dimension use of telephone to dimension elimination. Most of the patients were independent in the dimensions use of telephone and eating. The patients were most dependent in the dimensions elimination, which includes bladder and bowel management. Using assistive devices and car and house adaptations makes the patients more independent in ADL ( =assistive devices and #=house and car adaptations) (Figure 3). Assistive devices can either be applied to the hand or be handled with active grip function. The patients were more dependent in items including grip function visualized through linking the K–B Scale to the ICF and analyses with Napier's and Bendz's definition of grip function. This is most clearly seen in dressing the lower body (marked dark gray squares=arm/hand function) (Figure 3). In the majority of items where precision grip is a prerequisite, the patients were more dependent in parts of dimensions. This was most clearly seen in the dimension dressing in the case of putting on shoes, trousers, shirt, jacket, bra and in cutting nails (marked light gray squares=precision grips) (Figure 3). Assistive devices were used in 68% of the items and car and house adaptations were used in 11% of the items. Eighty-two percent of the 159 items required grip function and 22% of these items required precision grip. Assistive devices compensate for the loss of grip function in 57% of 159 items (Figure 3).
=assistive devices and #=house and car adaptations) (Figure 3). Assistive devices can either be applied to the hand or be handled with active grip function. The patients were more dependent in items including grip function visualized through linking the K–B Scale to the ICF and analyses with Napier's and Bendz's definition of grip function. This is most clearly seen in dressing the lower body (marked dark gray squares=arm/hand function) (Figure 3). In the majority of items where precision grip is a prerequisite, the patients were more dependent in parts of dimensions. This was most clearly seen in the dimension dressing in the case of putting on shoes, trousers, shirt, jacket, bra and in cutting nails (marked light gray squares=precision grips) (Figure 3). Assistive devices were used in 68% of the items and car and house adaptations were used in 11% of the items. Eighty-two percent of the 159 items required grip function and 22% of these items required precision grip. Assistive devices compensate for the loss of grip function in 57% of 159 items (Figure 3).

The proportion of independent patients in 159 items divided into the dimensions use of telephone, eating, mobility, hygiene, dressing and elimination in the Klein–Bell ADL Scale. (n=55). ( )=number of items included in parentheses, ( )=assistive devices, (#)=house and car adaptations, marked dark grey squares=arm function and hand function, that is grasp abilities needed to perform the item(s), marked light grey squares=precision grips, that is manipulation needed to perform the item(s)
)=assistive devices, (#)=house and car adaptations, marked dark grey squares=arm function and hand function, that is grasp abilities needed to perform the item(s), marked light grey squares=precision grips, that is manipulation needed to perform the item(s)
Correlation between the K–B Scale and upper extremity function
The raw sum score for the patients ranged from 42 to 456 in the K–B Scale and the UEMS ranged from 23 to 184. There was a moderate correlation between the raw sum score in the K–B Scale and the UEMS for shoulder muscles to intrinsic muscles rs=0.63 (P<0.01) (Figure 4). The patients' sensibility ranged from no sensory function in all fingers to full sensory function in all finger according to 2PD test divided into ASIA sensory level. There was a moderate correlation between the raw sum score in the K–B Scale and the 2PD test with ⩽10 mm in number of fingers rs=0.68 (P<0.01).

Relationship between the patients' raw sum score in the Klein–Bell ADL Scale and UEMS from shoulder to intrinsic muscles. The Spearman's rank correlation coefficient was rs=0.63 (P<0.01). (n=53)
Analysis of the weight scheme in the K–B Scale
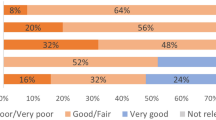
The proportion of patients who carried out the item independently was calculated for each item. These proportions were grouped according to the K–B weight scheme; simple, average complex and complex. Simple items (25th–75th percentiles) ranged between 46 and 83% (median of 60%), average complex items between 35 and 77% (median of 44%) and complex items between 27 and 79% (median of 53%) (Figure 5).

The proportion of patients who independently performed items classified as simple, average complex and complex items in the Klein–Bell ADL Scale. (n=55)
The proportions of items in the K–B Scale performed independently by the patients were calculated for each of the three weight levels. The mean percentage groups were 64% in the simple items, 55% in the average complex items and 61% in the complex items. The proportions were thereafter tested with regard to differences between the weight levels in the K–B Scale (Table 2). The comparison between the weight levels showed that there was a difference in complexity between simple items and average complex items, the difference were 8.5 percentage units and there was a inverted difference in complexity between average complex items and complex items, and the difference were 5.6 percentage units and both the comparisons between the weight levels were significant. The comparison between simple items and complex items showed no statistical significant difference, the differences were 2.9 percentage units (Table 2).
Linking the K–B Scale to investigate grip function
Linking the K–B Scale to the ICF has together with Napier's definition and Bendz's description of grip function shown that the need for arm and hand function, that is, grasp ability, is included in all three levels in the K–B Scale's weight scheme. The items included either precision grips or power grips or a combination of the two. Simple items include items that either prepare or terminate an activity. Both average complex items and complex items involve performing or continuing an activity with static or dynamic grasp patterns. Precision grip (manipulation), a dynamic grasp ability was more common in average hard items.
Analyses of the structural properties in the K–B Scale
The analysis of the structural properties in the K–B Scale showed problems in 46 of 170 items during the measurement process. The distribution of these items was as follows; 34 items did not make any differences in functional limitations, that is, the items included different assessment alternatives owing to the formulation of the items operational criteria. The majority of the 34 items were found in dimensions of elimination and mobility. The assessment alternatives ranged between being independent in ADL without assistive devices and being independent with assistive devices. Seven items that included assessment of extra devices were not relevant for cervical SCI patient. Five functional items (bladder and bowel incontinence, chewing and swallowing food and swallowing liquids) showed a ceiling effect, that is, all patients were assessed as independent.
Discussion
The main results of this study show that the K–B Scale discriminated cervical SCI patients' ability to carry out basic ADL. For cervical SCI patients, only the analysis with raw sum score was useful. The K–B Scale can be used to assess basic ADL in cervical SCI patients in spite of the diversity in the functional levels, that is, differences in upper extremity function and differences in ability to be mobile. The K–B Scale measures basic ADL divided into essential components (items) of an activity. This is an advantage over other known ADL scales19, 39, 40 as it makes it possible to detect problematic items within dimensions and thus makes it a better tool for target interventions in ADL in patients with cervical SCI regardless of functional level.
Correlation between the K–B Scale and upper extremity function
Earlier studies have shown that upper extremity function and movement, that is, in transfer and push-up motions is decisive in the process of gaining independence in ADL.41, 42, 43 The patients' level of independence in ADL in the present study ranged from dependence in all dimensions except in items including eating and using the telephone to independence in all areas with the exception of items including precision grip. Patients used assistive devices and house and car adaptations to increase their level of independence; however, assistive devices cannot fully compensate for loss of grip function. This is most apparent in dressing in the case of putting on socks, shoes and pants, where active grip function is needed to handle assistive devices. According to Marino et al10 motor level and UEMS plays an important role in predicting ADL. In this study, the patients' motor levels and UEMS between right and left arm was heterogeneous. The relationship between the patient's level of independence in ADL and the UEMS was moderate in this study. Earlier studies5, 10 have shown that motor level is one determinant of independence in ADL. However, motor performance relies on sensory feedback,44 which has been shown to be important in controlling arm, hand and finger movements45, 46, 47 and cervical SCI patients with sensory-deficient hands have to rely on visual control of the hands to be active in daily life.48 Cutaneous feedback is an essential element in manipulation tasks, but this has not been easy to compare with performance in daily activity49 and earlier studies50, 51 have shown that sensory level seems to influence the patients' level of independence in ADL. The relationship between the patient's level of independence in ADL and the 2PD test was a moderate in this study. However, this study was not large enough to investigate how sensory function adds to the variance of ADL performance explained by UEMS. Other factors such as gender, age, body mass and time since injury,7, 8 together with factors in the environment,52 also influence the variance in the performance of ADL. These factors must be taken into consideration in the assessment of the cervical SCI patient's level of independence in ADL. For this reason, the patient's actual performance in ADL was assessed in the present study. The UEMS and the 2PD test have shown that most patients in the present study lacked full hand function, that is, they lacked the capability to grasp, to support and to manipulate, and that they also lacked sensory capability. Even though cervical SCI patients are resourceful and use compensatory strategies to maximize the use of their hand function,53 the results of this and earlier studies4, 41, 54 show that the impaired hand function will ultimately influence independence in ADL.
Impairment-specific dimensions in the K–B Scale
Earlier studies39, 55 have suggested measuring impairment-specific dimensions within ADL scales. A connection between function and activity in the items operational criteria has been established through linking the K–B Scale to the ICF and using Napier's definition and Bendz's description of grip function. Because of the many items it includes, the K–B Scale has the potential to be divided into impairment-specific items even for arm and grip function, in contrast to the Functional Independence Measure (FIM™),39 which divides motor FIM™ into only two sub scales, the upper and lower body. This approach to connect arm and hand function to basic ADL might give an understanding of the grasp abilities needed to perform an activity and might also explain why some items are more difficult to carry out than others. With these attributes, the K–B Scale can be a useful ADL instrument in connection with reconstructive hand surgery in cervical SCI patients.
Weight scheme in the K–B Scale versus arm and hand function
The K–B Scale20, 21 which is a generic instrument has been stated to be applicable across diseases and disorders but the results in this study did not correspond to the original construction of the complexity of the items according to the weight scheme in the K–B Scale.20, 21 There was an inverted difference in the complexity between average complex and complex items and there was no significant difference between simple and complex items. This might be due to the fact that all three levels, simple, average complex and complex, include items that require grasp abilities – power grip or precision grip or a combination of both, using one and two-hand grasps – to be considered independent in ADL.
Assessment of basic ADL in cervical SCI patients using a weight scheme where the complexity of the items is the same for patients (regardless of diagnosis) has been shown not to function. However, it might be applicable for patients with other diseases or disorders who have the same problems to perform ADL as stated in the original weight scheme in the K–B Scale.20, 21
It has been questioned in earlier studies whether it is worth the effort to weight items because weights may only create complexity in scoring. Furthermore, patients who are independent tend to score high on all items, and the opposite applies to those patients who score low on all items, regardless of whether weights are used.56 The solution might be to let the guiding principle concerning item complexity be reflected by the patients' choice of categories in the K–B Scale, as arm and hand function seems to play a crucial role in the independence of the patients in ADL.
Analyses of the structural properties in the K–B Scale
A generic instrument would provide an opportunity to compare patients across disorders, diseases and interventions but would on the other hand reduce the specificity of the scale.56 Earlier studies have shown that diagnosis-specific scales such as the Spinal Cord Independence Measure (SCIM)40 and the QIF19 are more sensitive to small changes in a patient's ability to perform ADL and therefore better reflect rehabilitation outcome in cervical SCI patients than FIM™.39 However, SCIM and QIF have items that lack requirements to assess important components of an activity. Compared to SCIM and QIF, the K–B Scale can measure basic daily activities in cervical SCI patients in greater detail.
However, using the K–B Scale in this study to assess ADL ability among cervical SCI patients has shown to be problematic with respect to the structural properties in the scale. Not applicable items in the scale contribute nothing but noise, which in turn lessens the usefulness of the scale.56 The use of the dichotomized categories of independence and dependence in the K–B Scale results in a loss of valuable information in the assessment. The dichotomized categories limit the patients' choice of response levels, which in turn leads to a loss of efficiency to discriminate patients' level of independence in the K–B Scale. It also reduces its correlation with other instruments or measures.56 The patients' level of independence, defined as the least to the most independent patient, is not clearly shown because assistive devices, use of wheelchair (especially in ambulation items) and differences in functional abilities in the K–B Scale are included in the items' operational criteria. This is together with the use of dichotomized categories a limitation in the K–B ADL Scale.
Raw sum score was used according to recommendations in the K–B Scale,20, 21 even though it makes it more difficult to interpret the results as patients can get the same scores in spite of different needs of assistance.57 The level of measurement for ADL scales is identified as categorical assessments which makes the use of sum score questionable and interpretations should therefore be made with statistical caution.58 Today there exist other approaches59, 60 for analyzing categorical assessments that better reflect the level of measurement than do the methods proposed in the K–B Scale.
Conclusion
The K–B Scale can be used to assess basic ADL with raw score and can discriminate between cervical SCI patients' ability from less to greater independence in ADL. The analyses have, however, shown inherent problems with the weight scheme. To become a useful tool, the K–B Scale's structural properties, its operational criteria in the items and its categories must be further investigated. Furthermore, its reliability in conjunction with arm and grip function in patients with cervical SCI has yet to be proven.
References
Waters RL, Adkins RH, Yakura JS, Sie I . Motor and sensory recovery following incomplete tetraplegia. Arch Phys Med Rehabil 1994; 75: 306–311.
Ditunno Jr JF, Young W, Donovan WH, Creasey G . The international standards booklet for neurological and functional classification of spinal cord injury. American Spinal Injury Association. Paraplegia 1994; 32: 70–80.
Lysack CL, Zafonte CA, Neufeld SW, Dijkers MP . Self-care independence after spinal cord injury: patient and therapist expectations and real life performance. J Spinal Cord Med 2001; 24: 257–265.
Welch RD, Lobley SJ, O'Sullivan SB, Freed MM . Functional independence in quadriplegia: critical levels. Arch Phys Med Rehabil 1986; 67: 235–240.
Burns AS, Ditunno JF . Establishing prognosis and maximizing functional outcomes after spinal cord injury: a review of current and future directions in rehabilitation management. Spine 2001; 26 (Suppl 24): S137–S145.
Dallmeijer AJ, van der Woude LH, Hollander PA, Angenot EL . Physical performance in persons with spinal cord injuries after discharge from rehabilitation. Med Sci Sports Exerc 1999; 31: 1111–1117.
Janssen TW, Dallmeijer AJ, Veeger DJ, van der Woude LH . Normative values and determinants of physical capacity in individuals with spinal cord injury. J Rehabil Res Dev 2002; 39: 29–39.
Yarkony GM, Roth EJ, Heinemann AW, Lovell L . Rehabilitation outcomes in C6 tetraplegia. Paraplegia 1988; 26: 177–185.
Krause JS, Broderick L . Outcomes after spinal cord injury: comparisons as a function of gender and race and ethnicity. Arch Phys Med Rehabil 2004; 85: 355–362.
Marino RJ, Rider-Foster D, Maissel G, Ditunno JF . Superiority of motor level over single neurological level in categorizing tetraplegia. Paraplegia 1995; 33: 510–513.
World Health Organization (WHO). International Classification of Functioning, Disability and Health (ICF). World Health Organization: Geneva 2001.
Cieza A, Geyh S, Chatterji S, Kostanjsek N, Ustun B, Stucki G . ICF linking rules: an update based on lessons learned. J Rehabil Med 2005; 37: 212–218.
Friden J, Ejeskar A, Dahlgren A, Lieber RL . Protection of the deltoid to triceps tendon transfer repair sites. J Hand Surg [Am] 2000; 25: 144–149.
Ejeskar A, Dahlgren A, Friden J . Split distal flexor pollicis longus tenodesis: long-term results. Scand J Plast Reconstr Surg Hand Surg 2002; 36: 96–99.
Ejeskar A, Dahllöf AG . Surgical rehabilitation in tetraplegia. In: Hurley R (ed). Rehabilitation of the Hand: Surgery and Therapy 4th edn. Mosby: St Louis 1995, pp 482–503.
Gansel J, Waters R, Gellman H . Transfer of the pronator teres tendon to the tendons of the flexor digitorum profundus in tetraplegia. J Bone Joint Surg Am 1990; 72: 427–432.
Rothwell A, Sinclair S . Upper limb tendon surgery for tetraplegia. Operative Orthopädie und Traumatologie 1997; 9: 199–212.
Sinnott KA, Dunn JA, Rothwell AG . Use of the ICF conceptual framework to interpret hand function outcomes following tendon transfer surgery for tetraplegia. Spinal Cord 2004; 42: 396–400.
Gresham GE, Labi ML, Dittmar SS, Hicks JT, Joyce SZ, Stehlik MA . The Quadriplegia Index of Function (QIF): sensitivity and reliability demonstrated in a study of thirty quadriplegic patients. Paraplegia 1986; 24: 38–44.
Klein RM, Bell B . The Klein–Bell ADL Scale Manual. University of Washington Medical School, Health Sciences Resources Centre SB-56: Seattle 1979.
Klein RM, Bell B . Self-care skills: behavioral measurement with Klein–Bell ADL scale. Arch Phys Med Rehabil 1982; 63: 335–338.
Law M, Usher P . Validation of the Klein–Bell activities of daily living scale for children. Can J Occup Ther 1988; 55: 63–68.
Titus MN, Gall NG, Yerxa EJ, Roberson TA, Mack W . Correlation of perceptual performance and activities of daily living in stroke patients. Am J Occup Ther 1991; 45: 410–418.
Bolding DJ, Llorens LA . The effects of habilitative hospital admission on self-care, self-esteem, and frequency of physical care. Am J Occup Ther 1991; 45: 796–800.
Kratz G, Soderback I, Guidetti S, Hultling C, Rykatkin T, Soderstrom M . Wheelchair users' experience of non-adapted and adapted clothes during sailing, quad rugby or wheel-walking. Disabil Rehabil 1997; 19: 26–34.
Medical Research Council. Aids to the Examination of the Peripheral Nervous System. HM Stationary Office: London 1976.
Moberg E . Two-point discrimination test. A valuable part of hand surgical rehabilitation, e.g. in tetraplegia. Scand J Rehabil Med 1990; 22: 127–134.
Cieza A et al. Linking health-status measurements to the international classification of functioning, disability and health. J Rehabil Med 2002; 34: 205–210.
Soderback I, Caneman G, Guidetti S, Hagsten BE . Klein–Bell ADL-Skala 1.0. Kind & Steinvik AB: Stockholm 1994.
Soderback I, Caneman G . Causes of dependence in personal care three years after stroke. Neurorehabilitation 1993; 3: 60–71.
Larsson EL, Aaro S, Oberg B . Activities and functional assessment 1 year after spinal fusion for paralytic scoliosis. Eur Spine J 1999; 8: 100–109.
Hagsten BE, Soderback I . Occupational therapy after hip fracture: a pilot study of the clients, the care and the costs. Clin Rehabil 1994; 8: 142–148.
Sandin C, Zachrisson G . ADL–Diagram 1.11 edn. Göteborg: Sandin Design 2003.
Klein RM, Bell B . The Klein–Bell ADL Scale Manual. University of Washington Medical School, Health Sciences Resources Centre SB-56: Seattle (undated).
Munro BH . Statistical Methods for Health Care Research 5th edn. Lippincott Williams & Wilkins: Philadelphia, Pa; London 2004.
Altman DG . Practical Statistics for Medical Research. Chapman and Hall: London 1991.
Napier JR . The prehensile movements of the human hand. J Bone Joint Surg Br 1956; 38-B: 902–913.
Bendz P . Systematization of the grip of the hand in relation to finger motor systems. A kinesiologic study using a new method for recording finger joint motions. Scand J Rehabil Med 1974; 6: 158–165.
Stineman MG, Jette A, Fiedler R, Granger C . Impairment-specific dimensions within the Functional Independence Measure. Arch Phys Med Rehabil 1997; 78: 636–643.
Catz A, Itzkovich M, Agranov E, Ring H, Tamir A . SCIM – Spinal Cord Independence Measure: a new disability scale for patients with spinal cord lesions. Spinal Cord 1997; 35: 850–856.
Fujiwara T, Hara Y, Akaboshi K, Chino N . Relationship between shoulder muscle strength and functional independence measure (FIM) score among C6 tetraplegics. Spinal Cord 1999; 37: 58–61.
Harvey LA, Crosbie J . Biomechanical analysis of a weight-relief maneuver in C5 and C6 quadriplegia. Arch Phys Med Rehabil 2000; 81: 500–505.
Gronley JK, Newsam CJ, Mulroy SJ, Rao SS, Perry J, Helm M . Electromyographic and kinematic analysis of the shoulder during four activities of daily living in men with C6 tetraplegia. J Rehabil Res Dev 2000; 37: 423–432.
Cohen HS . Neuroscience for Rehabilitation 2nd edn. Lippincott: Philadelphia 1999.
Gentilucci M, Toni I, Daprati E, Gangitano M . Tactile input of the hand and the control of reaching to grasp movements. Exp Brain Res 1997; 114: 130–137.
Collins DF, Knight B, Prochazka A . Contact-evoked changes in EMG activity during human grasp. J Neurophysiol 1999; 81: 2215–2225.
Monzee J, Lamarre Y, Smith AM . The effects of digital anesthesia on force control using a precision grip. J Neurophysiol 2003; 89: 672–683.
Moberg E . The Upper Limb in Tetraplegia: A New Approach to Surgical Rehabilitation. Thieme: Stuttgart 1978.
Ebied AM, Kemp GJ, Frostick SP . The role of cutaneous sensation in the motor function of the hand. J Orthop Res 2004; 22: 862–866.
Curt A, Dietz V . Traumatic cervical spinal cord injury: relation between somatosensory evoked potentials, neurological deficit, and hand function. Arch Phys Med Rehabil 1996; 77: 48–53.
Maissel G, Cohen M . Pin sensation is significant for self care function in quadraplegia. J Am Paraplegia Soc 1993; 16: 86.
Law MC, Baum CM, Dunn W . Measuring Occupational Performance: Supporting Best Practice in Occupational Therapy. Slack: Thorofare, NJ 2001.
Johanson ME, Murray WM . The unoperated hand: the role of passive forces in hand function after tetraplegia. Hand Clin 2002; 18: 391–398.
Rogers JC, Figone JJ . Traumatic quadriplegia: follow-up study of self-care skills. Arch Phys Med Rehabil 1980; 61: 316–321.
Coster WJ, Haley SM, Andres PL, Ludlow LH, Bond TL, Ni PS . Refining the conceptual basis for rehabilitation outcome measurement: personal care and instrumental activities domain. Med Care 2004; 42 (Suppl 1): I62–I72.
Streiner DL, Norman GR . Health Measurement Scales: A Practical Guide to Their Development and Use. 3rd edn. Oxford University Press: Oxford 2003.
Eakin P . Assessments of activities of daily living: a critical review. Part 1. Br J Occup Ther 1989; 52: 11–15.
Bowling A . Measuring Health: A Review of Quality of Life Measurement Scales. 3rd edn. Open University Pr.: Buckingham 2005.
Sonn U, Svensson E . Measures of individual and group changes in ordered categorical data: application to the ADL staircase. Scand J Rehabil Med 1997; 29: 233–242.
Tesio L . Measuring behaviours and perceptions: Rasch analysis as a tool for rehabilitation research. J Rehabil Med 2003; 35: 105–115.
Acknowledgements
We thank Anna Ekman for valuable help with statistics. This study was supported by grants from the Norrbacka-Eugenia Foundation, The Swedish Association of Survivors of Traffic Accidents and Polio foundation (RTP), The Foundation of Sunnerdahls Handicap Fund, The Swedish National Association for Disabled Children and Young People (RBU), The Capio Foundation, The Council of Research and Development of Gothenburg and Southern Bohuslan.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Dahlgren, A., Karlsson, AK., Lundgren-Nilsson, Å. et al. Activity performance and upper extremity function in cervical spinal cord injury patients according to the Klein–Bell ADL Scale. Spinal Cord 45, 475–484 (2007). https://doi.org/10.1038/sj.sc.3101993
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101993
