
Abstract
Study design:
A case report of an epidermoid cyst in the conus medullaris with characteristic magnetic resonance imaging (MRI) findings.
Objective:
To describe an epidermoid cyst in the conus medullaris with characteristic MRI findings and point out these findings that correlated well with histologic findings.
Setting:
Taiwan.
Case report:
A 49-year-old man who suffered from pain and weakness in his right leg for 16 years. MRI showed a heterogeneous signal mass in the conus medullaris. The hyperintense signal area within the lesion may be attributed to the keratin content, whereas the hypointense signal area was related to calcification and soft-tissue component. The histologic findings were compatible with an epidermoid cyst.
Conclusion:
Epidermoid cysts in the conus medullaris must be considered in the differential diagnosis of mass lesions with long duration of related symptoms. The characteristic MRI findings are useful to differentiate epidermoid cysts from other tumors.
Similar content being viewed by others

Introduction
Spinal epidermoid cysts are rare and slow-growing benign lesions that may be congenital or acquired.1 Most cases are subdural and extramedullary; intramedullary epidermoid cysts are extremely rare.2 We report a case of an epidermoid cyst in the conus medullaris with characteristic magnetic resonance imaging (MRI) findings. These findings correlated well with histopathology.
Case report
A 49-year-old man suffered from a 16-year history of pain and weakness in his right leg following a falling accident. There was no open wound injury in this accident. The symptoms often subsided after rest. He was treated unsuccessfully by traditional medicine. His right calf weakness had become worse 1 month before admission.
Physical examination revealed hyperesthesia over the L5 level of the right leg, of which the myotome was reduced and ankle dorsiflexion was affected. Lower limb reflexes were normal bilaterally.
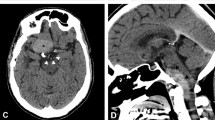
Plain X-ray films of the spine showed a mild posterior scalloping of the L2 vertebral body and degenerative change of the lumbar spine. MRI (1.5-T, Horizon LX, General Electric, WI, USA) showed a tumor mass in the conus medullaris (Figure 1a–e), measuring 6.0 × 1.2 cm2, between the L1 and L3 levels. A widened tumor–conus interface was noted. The tumor was shown by heterogeneous signal intensity on precontrast MRI images and some area of enhancement on postcontrast MRI images. In addition, mild bulging discs at L3-4 and L5-S1 were noted. There was a left paracentral protruded disc at L4-5 with subtle impingement upon left L5 nerve root. The clinical symptoms were not related to the degenerative disc disease.

(a) Sagittal T1-weighted image shows an intramedullary mass, extending from L1 to L3. The hyperintense signal areas (arrow) within the tumor and its wall (arrowhead) are consistent with keratin on histology. (b) On the T2-weighted image the tumor mass is heterogeneous, shown mainly by hypointensity (curved arrow). Note that some hypointense signal spots (arrows) are attributed to calcifications on histology. (c) On the gadolinium-enhanced T1-weighted image, some area of enhancement within the tumor (curved arrow) and its wall (arrows) was seen. (d) Axial T2-weighted image at L1-2 level shows areas of hyperintensity (curved arrow) and hypointensity (arrow) within the tumor. (e) On the gadolinium-enhanced image, obvious enhancement is noted at the T2-weighting hypointense area (arrow), suggestive vascular connective tissue. (f) Photomicrograph of the tumor mass (H&E, × 40). The lesion is filled with keratinous substance (arrowhead) with focal calcification (arrow). (g) Photomicrograph of the tumor mass near the cyst wall (H&E, × 200). The cyst is lined by benign keratinizing squamous epithelium with a fibrotic wall (arrow)
The patient received laminectomy from T11 to L3. After the dura was exposed, a well-encapsulated tumor mass was identified in the corda equina and conus medullaris. The tumor capsule adhered tightly to the thickened arachnoid membrane at L2. Brownish and greasy contents within the capsule were noted. The tumor was incompletely removed at its proximal end owing to firm adhesion to the roots and conus medullaris.
Histologically, the specimen contained, predominantly, a keratin substance with focal calcifications (Figure 1f and g). There were some tiny pieces of anucleated or mature squamous epithelium. The histological findings were compatible with an epidermoid cyst.
Discussion
Manno et al1 reviewed a series of 90 intraspinal epidermoid cysts from the literature; 39 of them were acquired and 51 were congenital. Acquired epidermoid cysts usually occur years after trauma including lumbar spinal punctures.3 Congenital spinal epidermoid cysts are believed to be related to inclusion of ectodermal tissue during closure of the neural tube between the third and fourth weeks of fetal life.1 Our patient had no known history of open wound trauma and, therefore, the tumor was thought to be congenital.
Epidermoid cysts most frequently occur in the thoracic region, especially between T5 and T8.2 Epidermoid cysts arising in the cervical spinal cord have not been reported. Roux et al2 reviewed 47 reported cases of the epidermoid cyst; only two of them originated from the conus medullaris. All 47 cases had a long duration of symptoms, ranging from 6 months to 53 years.
The stratified squamous epithelium forms the wall of the epidermoid cyst, which is supported by an outer layer of collagenous tissue. The process of desquamation and breakdown of keratin from the epithelial lining produces the contents of the cysts, which are rich in cholesterol crystals, triglyceride and fatty acids. The contents and the wall can be calcified.4 The growth rate approximates that of normal skin, in contrast to the much faster growth of most neoplasms.5 Malignant transformation is rare.2
MRI can show a wide variety of characteristics of the epidermoid cyst, which contain heterogeneous material in the central cavity.2, 6, 7 A thin rim of enhancement of the epidermoid cysts on gadolinium-enhanced MRI images has been inconsistently described.6, 8 Atypical imaging features are high density on CT images, a hyperintense signal on T1-weighted images, or a hypointense signal on T2-weighted MRI images.8 A spinal epidermoid cyst with diffusion-weighted MRI findings has been reported.9 The apparent diffusion coefficient (ADC) values indicated restricted diffusion within the mass.
In our case, on T1-weighted MRI, the hyperintense signal area within the lesion may be attributed to the keratin content, as proved by histopathology. Horowitz et al10 also suggested that the high content of triglycerides and unsaturated fatty acids in epidermoid cysts may contribute to the hyperintensity on T1-weighted images. Methemoglobin resulting from bleeding within the cyst could be another cause of the hyperintensity.11
Dunn et al12 reported a case with hemosiderin-laden macrophages in an intracranial epidermoid cyst, which corresponded with a hypointense signal area. In our case, some area of hypointensity on both the T1- and T2-weighted images may contribute to the histological findings of calcification. The disparity in signal intensity most likely reflects the variable lipid and protein composition of the lesions.13 The major area of hypointensity on T2-weighting turned out to be hyperintensity on gadolinium-enhanced images, suggestive of vascular connective tissue.11 The thin enhancing rim of epidermoid cysts is correlated with mature squamous epithelium and fibrotic tissue surrounding the cyst, as documented in our histopathology and in a previous study.11
Spinal dermoid cysts are similar to epidermoids in their squamous epithelial structure; however, dermoid cysts contain dermal appendages such as sweat glands and hair follicles. The cystic lesion of dermoids contains mainly fatty tissue that is shown as a hyperintense signal area on T1-weighted images, in contrast to the generally hypointense area of epidermoids.14 In spinal cystic neurilemmomas, the enhanced cystic wall is relatively thick and irregular, whereas the wall is thick or thin in some places of the epidermoid cyst. In enterogeneous cysts, the wall is extremely thin and does not show enhancement. The differences in the thickness of the wall reflect the number of layers of tumor cells.15
In summary, we present a case of a 49-year-old man with a long duration of related symptoms of being diagnosed of having epidermoid cyst in the conus medullaris with characteristic MRI findings. These findings correlated well with the histopathological findings.
References
Manno NJ, Uihlein A, Kernohan JW . Intraspinal epidermoids. J Neurosurg 1962; 19: 754–765.
Roux A, Mercier C, Larbrisseau A, Dube LJ, Dupuis C, Del Carpio R . Intramedullary epidermoid cyst of the spinal cord. J Neurosurg 1992; 76: 528–533.
Alves AM, Norrell H . Intramedullary epidermoid tumors of the spinal cord. Report of a case and review of the literature. Int Surg 1970; 54: 239–243.
Russell DS, Rubinstein LJ . Pathology of Tumors of the Nervous System. Williams and Wilkins: Baltimore 1989.
Alvord EC . Growth rates of epidermoid tumors. Ann Neurol 1977; 2: 367–370.
Hatfield MK, Udesky RH, Strimling AM, Kim BH, Silbergleit R . MR imaging of a spinal epidermoid tumor. AJNR 1989; 10: S95–S96.
Visciani A, Savoiardo M, Balestrini MR, Solero CL . Iatrogenic intraspinal epidermoid tumor: myelo-CT and MRI diagnosis. Neuroradiology 1989; 31: 273–275.
Gualdi GF, Di Biasi C, Trasimeni G, Pingi A, Vignati A, Maira G . Unusual MR and CT appearance of an epidermoid tumor. AJNR 1991; 12: 771–772.
Teksam M, Casey SO, Michel M, Benson M, Truwit CL . Intraspinal epidermoid cyst: diffusion-weighted MRI. Neuroradiology 2001; 43: 572–574.
Horowitz BL, Chari MV, James R, Bryan RN . MR of intracranial epidermoid tumors: correlation of in vivo imaging with in vitro C13 spectroscopy. AJNR 1990; 11: 299–302.
Debray MP, Ricolfi F, Brugieres P, Khalil A, Adle-Biassette H, Gaston A . Epidermoid cyst of the conus medullaris: atypical MRI and angiographic features. Neuroradiology 1996; 38: 526–528.
Dunn RC, Archer CA, Rapport RL, Looi LM . Unusual CT-dense posterior fossa epidermoid cyst. Case report. J Neurosurg 1981; 55: 654–656.
Phillips J, Chiu L . Magnetic resonance imaging of intraspinal epidermoid cyst: a case report. J Comput Assist Tomogr 1987; 11: 181–183.
Graham DV, Tampier D, Villemure JG . Intramedullary dermoid tumor diagnosed with the assistance of magnetic resonance imaging. Neurosurgery 1988; 23: 765–767.
Matsui H, Kanamori M, Yudoh K, Ohmori K, Yasuda T, Wakaki K . Cystic spinal cord tumors: magnetic resonance imaging correlated to histopathological findings. Neurosurg Rev 1998; 21: 147–151.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Lai, SW., Chan, W., Chen, CY. et al. MRI of epidermoid cyst of the conus medullaris. Spinal Cord 43, 320–323 (2005). https://doi.org/10.1038/sj.sc.3101673
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.sc.3101673
Keywords
This article is cited by
-
Intramedullary lesions of the conus medullaris: differential diagnosis and surgical management
Neurosurgical Review (2009)
