
Abstract
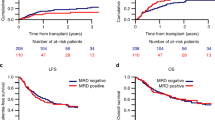
A total of 31 adult patients with AML entered in the EORTC/GIMEMA AML-10 trial, who received autologous stem cell transplantation (ASCT) after induction and consolidation chemotherapy, were prospectively evaluated for minimal residual disease (MRD) by multidimensional flow cytometry (MFC). Using a cutoff level of 3.5 × 10−4 leukemic cells pre-ASCT, 12 patients (39%) were stratified to MRD high-risk group and 19 (61%) into MRD low-risk group. During follow-up, all patients who were in the high-risk group relapsed at a median time of 7 months; in the low-risk group, five patients relapsed at a median time of 11 months and 14 remained in remission for 56 (range 7–80) months (P=0.00004). Longitudinal MFC determinations post-ASCT showed increased MRD levels in three of the five patients who underwent subsequent relapse, while disease recurrence was unpredicted in the remaining two cases. The pre-ASCT MRD status was the factor most strongly associated with relapse risk in the multivariate analysis (P=0.0014). We conclude that: (1) pre-ASCT MRD status predicts successful outcome in patients receiving ASCT; (2) high-dose chemotherapy conditioning regimen followed by ASCT has no impact on the unfavorable prognostic value of high pre-ASCT MRD level; and (3) sequential MRD monitoring post-ASCT may allow the prediction of impending relapse.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout


Similar content being viewed by others

References
Coustan-Smith E, Bhem FG, Sanchez J, Boyett JM, Hancock LM, Raimondi SC et al. Immunological detection of minimal residual disease in children with acute lymphoblastic leukemia. Lancet 1998; 351: 550–554.
Coustan-Smith E, Sancho J, Hancock ML, Boyett JM, Bhem FG, Raimondi SC et al. Clinical importance of minimal residual disease in childhood acute lymphoblastic leukemia. Blood 2000; 96: 2691–2696.
Coustan-Smith E, Sancho J, Hancock ML, Razzouk BI, Ribeiro RC, Rivera GK et al. Use of peripheral blood instead of bone marrow to monitor residual disease in children with acute lymphoblastic leukemia. Blood 2002; 100: 2399–2402.
San Miguel JF, Martinez A, Macedo A, Vidriales MB, Lopez-Berges C, Gonzalez M et al. Immunophenotyping investigation of minimal residual disease is a useful approach for predicting relapse in acute myeloid leukemia patients. Blood 1997; 90: 2465–2470.
San Miguel JF, Vidriales MB, López-Berges MC, Diaz-Mediavilla J, Gutiérrez N, Caòizo C et al. Early immunophenotypical evaluation of minimal residual disease in acute myeloid leukemia identifies different patient risk groups and may contribute to postinduction treatment stratification. Blood 2001; 98: 1746–1751.
Venditti A, Buccisano F, Del Poeta G, Maurillo L, Tamburini A, Cox C et al. Level of minimal residual disease after consolidation therapy predicts outcome in acute myeloid leukemia. Blood 2000; 96: 3948–3952.
Venditti A, Tamburini A, Buccisano F, Del Poeta G, Maurillo L, Panetta P et al. Clinical relevance of minimal residual disease detection in adult acute myeloid leukemia. J Hematother 2002; 11: 349–357.
Campana D, Pui C-H . Detection of minimal residual disease in acute leukemia: methodological advances and clinical significance. Blood 1995; 85: 1416–1434.
Terstappen LWMM, Loken MR . Myeloid cell differentiation in normal bone marrow and acute myeloid leukemia assessed by multi-dimensional flow cytometry. Ann Cell Path 1990; 2: 229–240.
Kaplan EL, Meier P . Non parametric estimations from incomplete observations. J Am Stat Assoc 1958; 53: 457–461.
Cheason BD, Cassileth PA, Head DR, Schiffer CA, Bennett JM, Bloomfield CD et al. Report of the National Cancer Institute-sponsored workshop on definitions of diagnosis and response in acute myeloid leukemia. J Clin Oncol 1990; 8: 813–819.
Burnett AK . Current controversies: which patients with acute myeloid leukemia should receive a bone marrow transplantation. An adult treater's view. Br J Haematol 2002; 118: 357–364.
Zittoun RA, Mandelli F, Willemze R, de Witte T, Labar B, Resegotti R et al. Autologous or allogeneic bone marrow transplantation compared with intensive chemotherapy in acute myelogenous leukemia. EORTC/GIMEMA. N Engl J Med 1995; 332: 217–223.
Harousseau JL, Cahn JY, Pignon B, Witz F, Milpied N, Delain M et al. Comparison of autologous bone marrow transplantation and intensive chemotherapy as postremission therapy in adult acute myeloid leukemia (GOLEAM). Blood 1997; 90: 2978–2986.
Burnett AK, Goldstone AH, Stevens RM, Hann IM, Rees JK, Gray RG et al. Randomised comparison of addition of autologous or allogeneic bone marrow transplantation to intensive chemotherapy for acute myeloid leukaemia in first remission: results of MRC AML10 trial. UK MRC and CLWP. Lancet 1998; 351: 700–708.
Cassileth PA, Harrington DP, Appelbaum FR, Lazarus HM, Rowe JM, Paietta E et al. Chemotherapy compared with autologous or allogeneic bone marrow transplantation in the management of acute myeloid leukemia in first remission. N Engl J Med 1998; 339: 1649–1656.
Suciu S, Mandelli F, de Witte T, Zittoun R, Gallo E, Labar B et al. Allogeneic compared to autologous stem cell transplantation in the treatment of patients <46 years old with AML in first CR: an intention to treat analysis of the EORTC/GIMEMA AML10 trial. Blood 2003 first edition paper.
Sievers EL, Appelbaum FR, Spielberg RT, Forman SJ, Flowers D, Smith FO et al. Selective ablation of acute myeloid leukemia using antibody-targeted chemotherapy: a phase I study of an anti-CD33 calicheamicin immunoconjugate. Blood 1999; 93: 3678–3684.
Meloni G, Trisolini SM, Capria S, Torelli GF, Baldacci E, Torromeo C et al. How long can we give interleukin-2? Clinical and immunological evaluation of AML patients after 10 or more years of IL2 administration. Leukemia 2002; 16: 2016–2018.
Meloni G, Diverio D, Vignetti M, Avvisati G, Capria S, Petti MC et al. Autologous bone marrow transplantation for acute promyelocytic leukemia in second remission: prognostic relevance of pretransplant minimal residual disease assessment by reverse transcription-polymerase chain reaction of PML/RARa. Blood 1997; 90: 1321–1325.
Keating ES, Suciu S, De Witte T, Zittoun R, et al. EORTC Leukemia Group, GIMEMA Leukemia Group. The stem cell mobilizing capacity of patients with acute myeloid leukemia in complete remission correlates with relapse risk: results of the EORTC-GIMEMA AML 10 trial. Leukemia 2003; 17: 60–67.
Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Venditti, A., Maurillo, L., Buccisano, F. et al. Pretransplant minimal residual disease level predicts clinical outcome in patients with acute myeloid leukemia receiving high-dose chemotherapy and autologous stem cell transplantation. Leukemia 17, 2178–2182 (2003). https://doi.org/10.1038/sj.leu.2403138
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.leu.2403138
Keywords
This article is cited by
-
Different effects of thymoglobulin on acute leukemia with pre-transplant residual blasts in HLA mismatch transplantation
International Journal of Hematology (2023)
-
Classifying AML patients with inv(16) into high-risk and low-risk relapsed patients based on peritransplantation minimal residual disease determined by CBFβ/MYH11 gene expression
Annals of Hematology (2019)
-
Impact of pre-transplantation minimal residual disease determined by multiparameter flow cytometry on the outcome of AML patients with FLT3-ITD after allogeneic stem cell transplantation
Annals of Hematology (2018)
-
Pre-transplant persistence of minimal residual disease does not contraindicate allogeneic stem cell transplantation for adult patients with acute myeloid leukemia
Bone Marrow Transplantation (2017)
-
Comparable outcomes between autologous and allogeneic transplant for adult acute myeloid leukemia in first CR
Bone Marrow Transplantation (2016)
