
Abstract
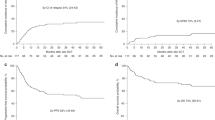
Clinical outcome of 47 consecutive patients with advanced HD who underwent ASCT in our Department was analyzed retrospectively. Median age was 28 years (28 males and 19 females). At transplant, 15 (32%) patients were in CR (five in first CR after two chemotherapy regimens and 10 in second CR), eight (17%) in PR (seven without a prior CR), 22 (51%) had relapsing disease (19 with sensitive relapse) and two had primary refractory disease. The CVB regimen with two different schedules was used: 22 (47%) patients received standard CBV (CY 6 g/m2, BCNU 300 mg/m2 and etoposide 600 mg/m2) and 25 (53%) received an increased CBV dose (CY 7.2 g/m2, BCNU 440 mg/m2 and etoposide 2 g/m2). Antitumor response for 28 evaluable patients was similar for both CBV regimens: 87 and 75% (P = 0.39). At 7.2 years, actuarial overall survival (OS), progression-free survival (PFS) and event-free survival (EFS) for the whole series were 51.7±8%, 34±9% and 28±8%, with a median follow-up for the surviving patients of 3 years (0.7–7.6). No differences in these survival functions according to the CBV regimen used were observed (P = 0.57). A history of a prior CR (P = 0.003), duration of first CR >1 year (P = 0.04), absence of bulky nodal disease at transplant (P = 0.054), absence of extranodal disease at transplant (P = 0.01), and a CR status at transplant (P = 0.0006) were associated with a better PFS on univariant analysis. On multivariate analysis, only CR status at transplant remained significant (P = 0.05). When patients in second CR at transplant and those in first sensitive relapse were analyzed separately, no differences in clinical characteristics or in treatment received pretransplant were observed; however, PFS was significantly different (P = 0.01). In conclusion, CR status at transplant is useful in identifying ‘good risk’ patients and is necessary to obtain the greatest benefit from ASCT independent of the CBV regimen used.
This is a preview of subscription content, access via your institution
Access options
Subscribe to this journal
Receive 12 print issues and online access
$259.00 per year
only $21.58 per issue
Buy this article
- Purchase on Springer Link
- Instant access to full article PDF
Prices may be subject to local taxes which are calculated during checkout
Similar content being viewed by others


Author information
Authors and Affiliations
Rights and permissions
About this article
Cite this article
Arranz, R., Tomás, J., Gil-Fernández, J. et al. Autologous stem cell transplantation (ASCT) for poor prognostic Hodgkin’s disease (HD): comparative results with two CBV regimens and importance of disease status at transplant. Bone Marrow Transplant 21, 779–786 (1998). https://doi.org/10.1038/sj.bmt.1701186
Received:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.bmt.1701186
Keywords
This article is cited by
-
Intensive conditioning regimen of etoposide (VP-16), cyclophosphamide and carmustine (VCB) followed by autologous hematopoietic stem cell transplantation for relapsed and refractory Hodgkin's lymphoma
Bone Marrow Transplantation (2008)
-
High-dose CEB vs BEAM with autologous stem cell transplant in lymphoma
Bone Marrow Transplantation (2004)
-
Autologous stem cell transplantation for Hodgkin's disease: busulfan, melphalan and thiotepa compared to a radiation-based regimen
Bone Marrow Transplantation (2003)
-
Autotransplants for Hodgkin's disease in first relapse or second remission: a report from the autologous blood and marrow transplant registry (ABMTR)
Bone Marrow Transplantation (2001)
-
Autologous stem cell transplantation for advanced Hodgkin's disease in children
Bone Marrow Transplantation (2000)
