
Abstract
Previous neuroimaging studies of major depression have not controlled for the presence of personality disorders characterized by impulsive aggressive behavior, such as borderline personality disorder (BPD). Using positron emission tomography (PET), we studied regional glucose uptake in response to fenfluramine (FEN) in depressed subjects with BPD (n=11) and depressed patients without Cluster B Axis II disorders (n=8). Subjects were scanned while medication-free after a single blind placebo administration and after FEN on a second day. Brain responses were measured by PET imaging of [18F]fluorodeoxyglucose (FDG) and serial prolactin levels. Scans were compared at a voxel level using statistical parametric mapping. Correlations of changes in relative regional cerebral uptake (rCMRglu) with clinical measures were assessed. Depressed borderline patients had greater relative activity in parietotemporal cortical regions (BA 40, BA 22, and BA 42) before and after FEN activation compared to those without BPD. They also had less relative uptake in the anterior cingulate cortex (BA 32) at baseline compared to depressed patients without BPD and FEN abolished this difference. Impulsivity was positively correlated with rCMRglu in superior and middle frontal cortex (BA 6 and 44). Hostility was positively correlated with rCMRglu in temporal cortical regions (BA 21 and 22). In conclusions, borderline pathology in the context of a Major Depressive Disorder is associated with altered activity in parietotemporal and anterior cingulate cortical regions. Controlling for the presence of BPD in future imaging studies of mood disorders may elucidate similarities and differences in regional serotonergic function in these two often comorbid disorders.
Similar content being viewed by others

INTRODUCTION
A lifetime history of mood disorder is more common in borderline personality disorder (BPD) than in other personality disorders (Bunce and Coccaro, 1999). Indeed, Zanarini et al (1998) noted an 83% lifetime prevalence of Major Depressive Disorder (MDD) in BPD patients. Thus, the two disorders often occur together. Apart from high rates of comorbidity, BPD and MDD both appear to be associated with low serotonergic activity (Coccaro et al, 1989; Oxenkrug, 1979; Siever et al, 1984). Although this shared serotonin abnormality may be related to a history of suicide attempt (Asberg, 1997) or impulsive aggression (Brown et al, 1979), we have shown an additive deficiency in the prolactin response to fenfluramine (FEN) due to the presence of major depression, BPD, and a history of serious suicide attempts (Malone et al, 1996). However, this serotonergic deficiency may not just be additive; it may also involve different neuroanatomical locations of serotonin innervation.
Neuroimaging studies permit anatomical localization of such abnormalities in vivo and can provide regional central nervous system functional data when used in conjunction with a serotonergic challenge. Serotonergic challenge with an agent such as FEN has utility in the delineation of the underlying psychopathology of affective disorders and borderline personality disorders since it is likely that serotonergic dysfunction associated with these disorders has both elements related to resting serotonergic tone as well as responsivity to external stressors or provocations. Moreover, it is likely that serotonergic dysfunction involves different neurocircuits in these two frequently comorbid conditions (see Mayberg et al (1999) and New et al (2002) for review).
Although previous neuroimaging studies of BPD mostly controlled for the presence of major depression (Juengling et al, 2003; Soloff et al, 2000; Soloff et al, 2003), brain imaging studies of major depression have not controlled for the presence of BPD. Studies focusing on the identification of serotonin abnormalities in MDD would benefit from controlling for potential confounds, such as the presence of other diagnoses associated with serotonergic dysfunction, as is the case with BPD. Such an approach can more accurately identify the neuroanatomical location of serotonergic abnormalities specific to MDD.
This study used positron emission tomography (PET) of regional cerebral uptake of [18F]fluorodeoxyglucose (rCMRglu) in response to serotonin elevation after an acute FEN challenge, relative to placebo challenge. With this methodology, we examined regional brain serotonergic function in major depression with comorbid BPD in comparison to major depression without BPD. In addition to comparing the two groups, we examined the effect of measures of impulsivity, hostility, and aggression on central serotonergic response as measured by rCMRglu after FEN. We hypothesized that the presence of BPD in patients with MDD would have a significant effect on cortical activity in the orbitofrontal and anterior cingulate regions, areas that play a central role in the regulation of aggressive and impulsive behavior and that these regions would be demonstrably associated with measures of these traits. To our knowledge, this is the first study of glucose metabolism in response to FEN in major depression that controls for comorbid BPD.
METHODS
Subjects
A total of 19 female subjects diagnosed with a Major Depressive Episode were included in this study. Informed consent was obtained from all subjects after a complete description of the study was provided. Eight did not have BPD or other cluster B Axis II disorder, and 11 had comorbid BPD. All but one patient with comorbid BPD were right-handed. Analyses conducted excluding this subject did not change results, so the data were preserved in the sample. Axis I diagnosis was assessed through the Structured Clinical Interview for DSM III R, Patient version (SCID-P) (Spitzer et al, 1990) and Axis II diagnosis was assessed with the SCID II-P interview (First et al, 1996). All subjects had MRI examinations and had no radiological evidence of neurological pathology. Exclusion criteria included active medical illness based on history, physical examination, and standard laboratory tests including liver function tests, hematological profile, thyroid function test, urinalysis, and toxicology; substance dependence in the last 6 months or substance abuse in the last 2 months; and pregnancy.
Measures
Depression was rated using the 17-item Hamilton Depression Rating Scale (HAM-D) (Hamilton, 1960) and the Beck Depression Inventory (BDI) (Beck et al, 1961). The Buss–Durkee Hostility Inventory (BDHI) (Buss and Durkee, 1957) and Brown Goodwin Lifetime Aggression Scale (BG) (Brown et al, 1979) were used to rate hostility and aggression, and the Barratt Impulsivity Scale (BIS) (Barratt, 1965) rated impulsivity.
Medication Washout
All medications were discontinued for a minimum of 14 days prior to PET studies (6 weeks for fluoxetine and 1 month for oral antipsychotic). Only subjects failing an adequate trial of medication were withdrawn from antidepressants. During the washout period, subjects were allowed up to 3 mg of lorazepam daily. This was discontinued 24 h before the scan. Premenopausal female subjects were studied within 5 days after onset of menstruation and were not on oral contraceptives.
FEN Challenge
Subjects had PET studies on two consecutive days after fasting from midnight and throughout the challenge test as previously described (Mann et al, 1996b; Oquendo et al, 2003). They received placebo on the first day and FEN on the second day in a single blind design. This study was conducted prior to the removal of FEN from the US market. On each study day, an intravenous catheter was inserted at approximately 0800 hours and a solution of 5% dextrose and 0.45% saline was infused. Prolactin levels were drawn 15 min and immediately before FEN or placebo administration to ascertain baseline levels. An oral dose of approximately 0.8 mg/kg of dl-FEN (or identical pills containing placebo) was administered at about 0900 hours. Prolactin, FEN, and norfenfluramine levels were drawn hourly for 5 h after medication administration. Subjects remained awake during the procedure. Prolactin levels were ascertained by immunoradiometric assay (McBride et al, 1989, 1990). The lower level of sensitivity of the method is 0.3 ng/m with an interassay coefficient of variation of 4%. Prolactin response to FEN at each time point was calculated as the difference between the prolactin level on FEN day and the prolactin level at the corresponding time point on placebo day. These values were compared between depressed patients with and without borderline personality disorder. FEN and norfenfluramine levels were measured by a gas–liquid chromatography method (Krebs et al, 1984; Myers et al, 1994).
PET Studies
Since FEN effects peak about 3 h after administration, and in an attempt to capture the maximal response to FEN, a bolus injection of approximately 5 mCi [18F]FDG was administered 3 h after the administration of placebo or FEN. Subjects gazed at a uniform visual stimulus (cross hairs) in a dimmed room during the first 15 min of the [18F]FDG distribution phase. After another 15 min, subjects were transferred to the scanner where they lay supine. A custom-made thermoplastic mask was used to minimize head movement and obtain comparable head position on the two scan days. The head was positioned so that the lowest scanning plane was parallel to the canthomeatal line and approximately 1.0 cm above it and then the infrared light positions on the mask were marked. For the second study, the head was positioned as closely as possible to the first study by using the original mask with the same marks. A Siemens ECAT EXACT 47 scanner (in plane spatial resolution 5.8 mm, axial resolution 4.3 mm FWHM at center) was used to acquire a 60 min emission scan in 2D mode in a series of twelve 5-min frames. The attenuation correction was measured by a 15-min 68Ge/68Ga transmission scan. Images were reconstructed with a Shepp radial filter, cutoff frequency of 35 cycles per projection rays and a ramp axial filter, cutoff frequency of 0.5 s.
Image Analysis
Two types of comparisons were made. One type of comparison was of differences in rCMRglu response to FEN compared to response to placebo in the MDD group as well as in the MDD with BPD group. The second type of comparison was of differences in rCMRglu in the MDD group compared with the MDD with BPD subjects after placebo as well as a comparison of responses in the two groups after FEN. These differences were evaluated using Statistical Parametric Mapping (SPM 99), (SPM Web page, 2002, www.fil.ion.ucl.ac.uk/spm/software/spm99). Automated image coregistration (Woods et al, 1992) was used to align the 12 frames within each study (Mann et al, 1996b). The resulting summarized image was transformed into standard stereotaxic atlas space (Talairach and Tournoux, 1988). Each image was smoothed by applying an isotropic Gaussian kernel to increase the signal to noise ratio. Analysis of covariance was applied within each condition controlling for global CMRglu. For each group (MDD only and MDD with BPD), the adjusted mean rCMRglu and variance were computed at each voxel for both placebo day and FEN day. These were used to compute t-tests of the differences of the means between groups for each study day at each voxel, and converted to Z-scores for graphical display as parametric maps. All values were corrected for multiple comparisons by SPM based on ‘the theory of continuous random fields, assuming the statistic image to be a good lattice representation of an underlying continuous stationary random field. Results for the Euler characteristic lead to corrected p-values for each voxel hypothesis’ (SPM Web page, 2002, www.fil.ion.ucl.ac.uk/spm/software/spm99).
Analysis of Effects of Clinical Parameters on rCMRglu
We calculated Pearsons's correlations between proportionally normalized rCMRglu values generated for the placebo and FEN day and scores on the Barratt Impulsivity Scale, Brown Goodwin Aggression Scale, and Buss–Durkee Hostility Inventory.
RESULTS
Clinical Characteristics of Depressed Female Subjects with and without BPD
Table 1 describes the clinical and demographic characteristics of eight female patients with MDD and no Cluster B Axis II diagnosis and 11 depressed female patients with comorbid BPD. The two groups had comparable severity of current depression, and lifetime impulsivity, hostility, and aggression. Of 11 depressed patients with BPD, seven (64%) had a history of at least one suicide attempt. Of eight depressed patients without BPD, four (50%) had a history of suicide attempt, a difference that was not statistically significant (Table 1). Prolactin levels rose significantly after FEN administration compared to after placebo but there was no significant difference between the two diagnostic groups in prolactin response to FEN (p=0.62).
Effects of FEN Compared to Placebo on rCMRglu
Results below are of voxel-based analysis of rCMRglu (analysis of covariance controlling for glucose metabolic rate) after placebo (day 1) compared to after FEN (day 2) administration in each group.
MDD With BPD
No areas of higher rCMRglu after FEN relative to placebo were found in the group with MDD with BPD. Subjects with MDD and BPD had an area in the right medial temporal gyrus (BA 21) with lower rCMRglu after FEN than after placebo (Figure 1). This finding did not reach statistical significance (corrected p=0.067).

Subjects with major depressive disorder with BPD have an area of decreased rCMRglu after FEN activation relative to placebo.

MDD without BPD
There was no difference in rCMRglu after FEN compared to after placebo administration.
rCMRglu in MDD with BPD Compared to MDD without BPD on Each of Two Study Days
Comparisons of rCMRglu after placebo were made between the two groups. Similar comparisons were conducted after FEN administration.
Regions where MDD with BPD subjects showed higher rCMRglu than MDD without BPD subjects
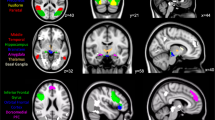
After placebo administration (Figure 2a), there was a single major area of higher rCMRglu on the right side in the group with MDD with BPD (cluster size 2042, corrected p=0.007) encompassing the superior temporal (BA 22 and 42) and inferior parietal gyrus (BA 40) when compared to the group with MDD only. After FEN (day 2) administration (Figure 2b), this area of greater rCMRglu (corrected p=0.013, cluster size 1740) became modestly smaller.

(a) Subjects with MDD with BPD have an area of greater rCMRglu compared to subjects with MDD without BPD at baseline (after placebo MMD+BPD>MDD). (b) Subjects with MDD with BPD have an area of greater rCMRglu compared to subjects with MDD without BPD after FEN (MMD+BPD>MDD). (c) Subjects with MDD with BPD have an area of less rCMRglu compared to subjects with MDD without BPD at baseline (placebo day) (MMD+BPD>MDD).

Regions where MDD with BPD subjects showed lower rCMRglu than MDD without BPD subjects
After placebo, a single area (Figure 2c) of lower rCMRglu (p=0.005) in the left anterior cingulate (BA 32) was noted in the comorbid MDD and BPD group when compared with the MDD only group. This group difference was abolished after FEN administration.
Relationship of PET Imaging Measures to Clinical Parameters
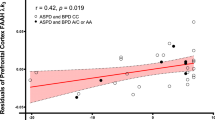
Pearson's correlations between clinical measures and rCMRglu are reported for both the placebo and the FEN administration days (Figure 3). After placebo administration, impulsivity correlated positively with rCMRglu in the right superior frontal gyrus (BA 6) and BA 44 and this association disappeared after FEN administration. At baseline (after placebo), hostility correlated positively with rCMRglu in the right middle temporal gyrus (BA 21) and remained after FEN administration. Measures of aggression did not correlate with rCMRglu in any regions on either study day.

Correlations of relative regional cerebral glucose metabolism rate and clinical variables after placebo (day 1) or FEN (day 2) administration.

DISCUSSION
This study used a serotonergic probe to assess differences in regional brain activity of depressed patients with and without BPD comorbidity. We hypothesized that comorbidity of BPD and MDD would have a significant effect on relative regional brain activity in the anterior cingulate and orbitofrontal areas. We found that depressed patients with comorbid borderline pathology have lower activity in the anterior cingulate area at baseline (placebo) when compared to patients with MDD only. This difference was not present after serotonin stimulation. In addition, depressed patients with borderline pathology had greater relative activity in parietotemporal regions at baseline and after serotonin stimulation, when compared to depressed patients without borderline pathology.
Anterior Cingulate in MDD with BPD Compared to MDD
We found lower regional activity in the anterior cingulate in depressed patients with BPD compared to depressed patients without BPD after placebo but not after FEN stimulation. Lesion studies suggest that control of aggression may be mediated by the anterior cingulate gyrus and orbitofrontal region (Butter et al, 1970; Grafman et al, 1996; Heinrichs, 1989; Raleigh et al, 1979). Functional neuroimaging studies of brain glucose metabolism in borderline and other aggressive and impulsive patients have also implicated the anterior cingulate area. In agreement with our findings, most studies of BPD found low relative glucose metabolism and regional cerebral blood flow (rCBF) in the anterior cingulate gyrus at rest (De La Fuente et al, 1997; Goyer et al, 1994). PET studies report that FEN responses are blunted in the orbitofrontal cortex and anterior cingulate gyrus (Siever et al, 1999) in impulsive aggressive subjects compared to healthy controls, as are m-CPP responses (New et al, 2002), although not all studies agree (Soloff et al, 2000). Moreover, a treatment study assessing decreases in aggressive behavior after a 12 week course of fluoxetine found that changes in cingulate and orbito-frontal glucose metabolism were correlated to clinical improvement, further supporting the importance of serotonergic function in these regions and the regulation of impulsive aggression (New et al, 2004).
We did not compare our subjects to normal controls, and thus cannot compare our results to the abovementioned studies directly. Our patients had BPD and comorbid with Major Depression. The presence of active depression in our subjects, which was not the case in samples studied by New et al (2002) for example, may have impeded detection of decreased responses to serotonergic challenge paradigms in anterior cingulate and orbitofrontal cortex in our study population because of the serotonergic hypofunction associated with Major Depression. Nonetheless, our finding supports the hypothesis that impulsive aggressive individuals such as those with BPD compared to nonimpulsive individuals have lower relative glucose metabolism in the anterior cingulate. This abnormality may be related to disinhibition via ungated input from downstream limbic/subcortical regions, such as the amygdala, that may predispose to aggression (for a review, see New et al, 2002). Of note, in our study, lower rCMRglu in the group with comorbid BPD was present during the placebo challenge and not during the FEN challenge, consistent with the notion that serotonin has serenic effects and may have a role in reducing impulsive aggression as was noted in a treatment study (New et al, 2004).
Orbitofrontal Cortex in MDD with BPD Compared to MDD
We did not find a difference in the orbitofrontal cortical area between depressed patients with BPD and MDD without BPD in contrast to findings from both lesion (Butter et al, 1970; Grafman et al, 1996; Heinrichs, 1989; Raleigh et al, 1979) and neuroimaging studies (De La Fuente et al, 1997; Goyer et al, 1994; New et al, 2002, 2004; Siever et al, 1999) that suggest a role for the orbitofrontal cortex in impulsive aggression. Our sample of depressed women with BPD did not differ significantly in terms of clinical measures of aggression and impulsivity from the depressed women without BPD (see Table 1). It is possible that a sample of more impulsive aggressive individuals in the BPD group may have permitted detection of such an effect. Alternatively, the effects of depression in this area may overpower those of impulsivity in BPD as some functional imaging studies have also suggested a role for the orbital prefrontal cortex in the pathophysiology of depression. For example, studies that examined abnormalities during a Major Depressive Episode and after various forms of treatment report normalization of orbitofrontal and anterior cingulate abnormalities with treatment (Baxter Jr et al, 1989; Bench et al, 1995; Brody et al, 1999; Buchsbaum et al, 1997; Mayberg et al, 2000, 2002). Indeed, Bremner et al (1997) found that depressed patients who were 6 weeks into a course of antidepressant treatment exhibited decreases in glucose metabolic rates in the orbitofrontal cortex and thalamus after a tryptophan-depletion-induced acute relapse compared to patients without depressive symptoms. A comparable pattern of abnormality in the orbitofrontal cortical region is seen in refractory depressed patients (Mayberg et al, 1997) and in patients with depression associated with neurological disorders (Bromfield et al, 1992; Mayberg et al, 1990, 1992). Mayberg et al (1999) suggested that mood provocation in patients with acute and remitted depression resulted in rCBF decrease in the medial orbitofrontal cortex BA 10/11, which was absent in healthy controls. She concluded that these regions might represent a site of vulnerability in patients with unipolar depression. Thus, the effects of the presence of Major Depression on lowering rCMRglu in orbital frontal regions may obviate our ability to detect effects of impulsive aggression.
Temporoparietal Cortical Region in MDD with BPD Compared to MDD Alone
In our study, depressed borderline patients had greater rCMRglu in parietotemporal cortical regions (BA 40, BA 22, BA 42) before and after FEN activation compared to depressed patients without BPD. One study using FDG found no differences in temporal glucose metabolism in subjects with BPD compared to healthy volunteers (De La Fuente et al, 1994). Similarly, a study using a FEN challenge design (Siever et al, 1999) has shown that impulsive aggressive patients have no differences in temporal rCMRglu compared to normal controls after placebo administration. However, also using a FEN challenge approach, Soloff et al (2000) found that borderline patients showed greater rCMRglu in the left superior temporal gyrus after placebo compared to normal controls, as was the case in our study. In contrast, using PET and alpha-[11-C] methyl-L-tryptophan (aMT), Leyton et al (2001) demonstrated lower aMT trapping in male and female patients with BPD compared with healthy controls in the superior temporal gyrus (BA 22) and the inferior parietal lobe BA 40 in men only, suggesting lower serotonin synthesis in those areas. Thus, studies of resting or post placebo temporal glucose metabolism in aggressive impulsive individuals and in BPD are not all in agreement. Studies using FEN challenge also show discrepant results after FEN administration. BPD patients are reported to have decreased response to FEN when compared to controls in left middle and superior temporal gyrus (BA 21–22), left inferior parietal lobe (BA 40), and left caudate body (Soloff et al, 2000). Similarly, impulsive aggressive patients have decreased regional metabolism in the right superior parietal cortex following FEN challenge compared with healthy volunteers (Siever et al, 1999). These two results are in contrast to ours. Since our comparison group was comprised of patients with MDD and impulsive aggression measures were similar in the two groups, it is possible that the observed increases in glucose metabolism in temporoparietal regions on both the placebo and FEN day are related to other characteristics of the BPD group. BPD is a heterogeneous disorder and impulsive aggression is only one of its features. Thus, this difference could relate to affective dysregulation, dissociative symptoms, rejection sensitivity, or other characteristics of the depressed BPD sample. We do not have data to address this possibility.
Of note, studies in MDD have implicated these regions as well. PET studies of glucose metabolism in depressed patients at rest have reported hypometabolism in parietal cortex (Austin et al, 1992; Biver et al, 1994) and temporal lobe (Post et al, 1987). Mayberg et al (1994) reported hypometabolism in the inferior parietal region (BA 40) along with the dorsal and ventral prefrontal cortex (BA 46), and the anterior cingulate (BA 24) in depressed patients. Mann et al (1996a) found blunted responses to FEN in prefrontal and parietotemporal cortex and Meyer et al (1998) in only parietotemporal regions. Taken together, studies suggest that depressed patients have lower activity in parietotemporal cortical areas, as is the case in most studies of impulsive patients.
Psychopathology in BPD
The principal dimensions that have been the focus of biological research in borderline pathology include impulsive aggression and affective dysregulation (Koenigsberg et al, 2001). Impulsive-aggression includes behaviors directed toward the self or others, such as self-injury, domestic violence, assault, suicide, and property destruction. In our study, hostility was associated with temporal cortical activity (BA 21) and impulsivity with right PFC areas (BA 6, BA 10) activity. Soloff et al (2003) reported significant reduction in FDG uptake in BPD subjects relative to healthy controls bilaterally in medial orbital frontal cortex, including BA 9, 10, and 11 and suggested that it may be associated with diminished regulation of impulsive behavior in BPD.
We were unable to find a relationship between aggression as measured by the Brown-Goodwin Aggression Scale and rCMRglu in any region. Previous imaging studies have implicated frontal and temporal brain region's metabolic changes to violence (Goyer et al, 1994; Volkow and Tancredi, 1987). Raine et al (1997) reported reduced glucose metabolism in PFC and posterior parietal cortex of a severely violent and mostly male sample. Our lack of findings may be due to the relatively low variance in aggression scores among our subjects.
Suicide attempts are often viewed as a subtype of aggressive behavior, and disturbance in the serotonergic system characterized by reduced CSF 5-HIAA has been associated with attempted or completed suicides in a variety of populations (Oquendo and Mann, 2000). The presence of suicidality in depressed patients has been suggested to influence neuroimaging findings in prefrontal cortex (Meyer et al, 1998). In our study given the similar proportion of suicide attempts in both groups, it is unlikely that the presence of a history of suicidal acts explains the observed metabolic differences in the ACG. The findings more likely reflect the association of these with aggressive impulsivity or other features of BPD such as affective instability. To our knowledge, there have been no neuroimaging studies of affective instability in personality disorders. However, depressive states can have characteristics that resemble those of BPD, such as the presence of suicidal acts, intense episodic dysphoria, a profound sense of emptiness, and increased affective lability. Just as there is an overlap in clinical presentation between borderline and depressed patients, neuroimaging studies also show significant overlap of changes in characteristic cortical regional activity patterns between MDD and BPD. Mayberg et al (1999) has proposed that changes in mood and not the overall diagnosis of MDD account for changes in activity patterns, and perhaps the same is true in BPD. Future imaging studies of depression should characterize impulsive aggressive subjects without MDD in order to obtain a fuller picture of brain activity pattern characteristic of major depression or depressed mood itself.
Limitations
This study has some limitations. First, the results require replication given the small sample size. Second, since the study included only female subjects, findings cannot be generalized to both sexes. However, regional CMRglu differences between men and women have not been consistently reported (Baxter Jr et al, 1989; Miura et al, 1990). Potential gender differences may exist in FEN activation of CMRglu as there is evidence of gender effects in serotonergic brain function, and rates of serotonin synthesis have been shown to differ by gender (Nishizawa et al, 1997). Moreover, gonadal hormones are known to affect serotonergic responsivity. We only studied women within 5 days of the onset of menses who were not on oral contraceptives. Nonetheless, hormonal variability may have affected our results despite our attempts to limit any such effects. Finally, this study did not make comparisons between the two studied patient populations and normal controls.
In conclusion, depressed borderline patients had lower rCMRglu in the anterior cingulate gyrus and this activity pattern appeared to be at least partially regulated by serotonin. They also showed higher rCMRglu in parietotemporal cortical region compared to depressed patients without BPD. These differences in the activity pattern suggest that the presence of comorbid BPD may have an impact on cortical activity and serotonin responsivity in depressed subjects.
References
Asberg M (1997). Neurotransmitters and suicidal behavior: the evidence from cerebrospinal fluid studies. Ann NY Acad Sci 836: 158–181.
Austin M-P, Dougall N, Ross M, Murray C, O'Carroll RE, Moffoot A et al (1992). Single photon emission tomography with 99mTc-exametazime in major depression and the pattern of brain activity underlying the psychotic/neurotic continuum. J Affect Disord 26: 31–43.
Barratt ES (1965). Factor analysis of some psychometric measures of impulsiveness and anxiety. Psycholog Rep 16: 547–554.
Baxter Jr. LR, Schwartz JM, Phelps ME, Mazziotta JC, Guze BH, Selin CE et al (1989). Reduction of prefrontal cortex glucose metabolism common to three types of depression. Arch Gen Psychiatry 46: 243–250.
Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J (1961). An inventory for measuring depression. Arch Gen Psychiatry 4: 53–63.
Bench CJ, Frackowiak RSJ, Dolan RJ (1995). Changes in regional cerebral blood flow on recovery from depression. Psychol Med 25: 247–261.
Biver F, Goldman S, Delvenne V, Luxen A, DeMaertelaer V, Hubain P et al (1994). Frontal and parietal metabolic disturbances in unipolar depression. Biol Psychiatry 36: 381–388.
Bremner JD, Innis RB, Salomon RM, Staib LH, Ng CK, Miller HL et al (1997). Positron emission tomography measurement of cerebral metabolic correlates of tryptophan depletion-induced depressive relapse. Arch Gen Psychiatry 54: 364–374.
Brody AL, Saxena S, Silverman DH, Alborzian S, Fairbanks LA, Phelps ME et al (1999). Brain metabolic changes in major depressive disorder from pre- to post-treatment with paroxetine. Psychiat Res 91: 127–139.
Bromfield EB, Altshuler L, Leiderman DB, Balish M, Ketter TA, Devinsky O et al (1992). Cerebral metabolism and depression in patients with complex partial seizures. Arch Neurol 49: 617–623.
Brown GL, Goodwin FK, Ballenger JC, Goyer PF, Major LF (1979). Aggression in human correlates with cerebrospinal fluid amine metabolites. Psychiatry Res 1: 131–139.
Buchsbaum MS, Wu J, Siegel BV, Hackett E, Trenary M, Abel L et al (1997). Effect of sertraline on regional metabolic rate in patients with affective disorder. Biol Psychiatry 41: 15–22.
Bunce SC, Coccaro E (1999). Factors differentiating personality-disordered individuals with and without a history of unipolar mood disorder. Depress Anxiety 10: 147–157.
Buss AH, Durkee A (1957). An inventory for assessing different kinds of hostility. J Consult Psychol 21: 343–349.
Butter CM, Snyder DR, McDonald JA (1970). Effects of orbital frontal lesions on the aggressive behaviors in rhesus monkeys. J Comp Physiol Psychol 72: 132–144.
Coccaro EF, Siever LJ, Klar HM, Maurer G, Cochrane K, Cooper TB et al (1989). Serotonergic studies in patients with affective and personality disorders. Correlates with suicidal and impulsive aggressive behavior. Arch Gen Psychiatry 46: 587–599.
De La Fuente JM, Goldman S, Stanus E, Vizuete C, Morlan I, Bobes J et al (1997). Brain glucose metabolism in borderline personality disorder. J Psychiat Res 31: 531–541.
De La Fuente JM, Lotstra F, Goldman S, Biver F, Luxen A, Bidaut L et al (1994). Temporal glucose metabolism in borderline personality disorder. Psychiatr Res Neuroimag 55: 237–245.
First MB, Spitzer RL, Gibbon M, Williams JMG, Benjamin L (1996). Structured Clinical Interview for DSM-IV Axis II Personality Disorders (SCID-II), (Version 2.0). Biometrics Research Department, New York State Psychiatric Institute: New York.
Goyer PF, Andreason PJ, Semple WE, Clayton AH, King AC, Compton-Toth BA et al (1994). Positron-emission tomography and personality disorders. Neuropsychopharmacology 10: 21–28.
Grafman J, Schwab K, Warden D, Pridgen A, Brown HR, Salazar AM (1996). Frontal lobe injuries, violence, and aggression: a report of the Vietnam head injury study. Neurology 46: 1231–1238.
Hamilton M (1960). A rating scale for depression. J Neurol Neurosurg Psychiatry 23: 56–62.
Heinrichs RW (1989). Frontal cerebral lesions and violent incidents in chronic neuropsychiatric patients. Biol Psychiatry 25: 174–178.
Juengling FD, Schmahl C, Hesslinger B, Ebert D, Bremner JD, Gostomzyk J et al (2003). Positron emission tomography in female patients with borderline personality disorder. J Psychiat Res 37: 109–115.
Koenigsberg HW, Harvey PD, Mitropoulou V, New AS, Goodman M, Silverman J et al (2001). Are the interpersonal and identity disturbances in the borderline personality disorder criteria linked to the traits of affective instability and impulsivity? J Pers Disord 15: 358–370.
Krebs HA, Cheng LK, Wright GJ (1984). Determination of fenfluramine and norfenfluramine in plasma using a nitrogen-sensitive detector. J Chromatogr Biomed Appl 310: 412–417.
Leyton M, Okazawa H, Diksic M, Paris J, Rosa P, Mzengeza S et al (2001). Brain regional alpha-[11C]methyl-L-tryptophan trapping in impulsive subjects with borderline personality disorder. Am J Psychiatry 158: 775–782.
Malone KM, Corbitt EM, Li S, Mann JJ (1996). Prolactin response to fenfluramine and suicide attempt lethality in major depression. Br J Psychiatry 168: 324–329.
Mann JJ, Malone KM, Diehl DJ, Perel J, Cooper TB, Mintun MA (1996a). Demonstration in vivo of reduced serotonin responsivity in the brain of untreated depressed patients. Am J Psychiatry 153: 174–182.
Mann JJ, Malone KM, Diehl DJ, Perel J, Nichols TE, Mintun MA (1996b). Positron emission tomographic imaging of serotonin activation effects on prefrontal cortex in healthy volunteers. J Cereb Blood Flow Metab 16: 418–426.
Mayberg HS, Brannan SK, Mahurin RK, Jerabek PA, Brickman JS, Tekell JL et al (1997). Cingulate function in depression: a potential predictor of treatment response. NeuroReport 8: 1057–1061.
Mayberg HS, Brannan SK, Tekell JL, Silva A, Mahurin RK, McGinnis S et al (2000). Regional metabolic effects of fluoxetine in major depression: serial changes and relationship to clinical response. Biol Psychiatry 48: 830–843.
Mayberg HS, Lewis PJ, Regenold W, Wagner HNJ (1994). Paralimbic hypoperfusion in unipolar depression. J Nucl Med 35: 929–934.
Mayberg HS, Liotti M, Brannan SK, McGinnis S, Mahurin RK, Jerabek PA et al (1999). Reciprocal limbic-cortical function and negative mood: converging PET findings in depression and normal sadness. Am J Psychiatry 156: 675–682.
Mayberg HS, Silva JA, Brannan SK, Tekell JL, Mahurin RK, McGinnis S et al (2002). The functional neuroanatomy of the placebo effect. Am J Psychiatry 159: 728–737.
Mayberg HS, Starkstein SE, Peyser CE, Brandt J, Dannals RF, Folstein SE (1992). Paralimbic frontal lobe metabolism in depression associated with Huntington's disease. Neurology 42: 1791–1797.
Mayberg HS, Starkstein SE, Sadzot B, Preziosi T, Andrezejewski PL, Dannals RF et al (1990). Selective hypometabolism in the inferior frontal lobe in depressed patients with Parkinson's disease. Ann Neurol 28: 57–64.
McBride PA, Anderson GM, Hertzig ME, Sweeney JA, Kream J, Cohen DJ et al (1989). Serotonergic responsivity in male young adults with autistic disorder. Arch Gen Psychiatry 46: 213–221.
McBride PA, Tierney H, DeMeo M, Chen J-S, Mann JJ (1990). Effects of age and gender on CNS serotonergic responsivity in normal adults. Biol Psychiatry 27: 1143–1155.
Meyer JH, Kennedy S, Brown GM (1998). No effect of depression on [15O]H2O PET response to intravenous d-fenfluramine. Am J Psychiatry 155: 1241–1246.
Miura SA, Schapiro MB, Grady CL, Kumar A, Salerno JA, Kozachuk WE (1990). Effect of gender on glucose utilization rates in healthy humans: a positron emission tomography study. Neurosci Res 27: 500–504.
Myers JE, Mieczkowski TA, Perel J, Abbondanza DM, Cooper TB, Mann JJ (1994). Abnormal behavioral responses to fenfluramine in patients with affective and personality disorders: correlation with increased serotonergic responsivity. Biol Psychiatry 35: 112–120.
New AS, Buchsbaum MS, Hazlett EA, Goodman M, Koenigsberg HW, Lo J et al (2004). Fluoxetine increases relative metabolic rate in prefrontal cortex in impulsive aggression. Psychopharmacology (Berlin) 176: 451–458.
New AS, Hazlett EA, Koenigsberg H, Platholi J, Silverman J, Siever LJ (2002). Blunted prefrontal cortical 18 fluorodeoxyglucose positron emission tomography response to metachlorophenylpiperazine in impulsive aggression. Arch Gen Psychiatry 59: 621–629.
Nishizawa S, Benkelfat C, Young SN, Leyton M, Mzengeza S, De Montigny C et al (1997). Differences between males and females in rates of serotonin synthesis in human brain. Proc Natl Acad Sci USA 94: 5308–5313.
Oquendo MA, Mann JJ (2000). The biology of impulsivity and suicidality. Psychiatr Clin North Am 23: 11–25.
Oquendo MA, Placidi GP, Malone KM, Campbell C, Keilp J, Brodsky B et al (2003). Positron emission tomography of regional brain metabolic responses to a serotonergic challenge and lethality of suicide attempts in major depression. Arch Gen Psychiatry 60: 14–22.
Oxenkrug GF (1979). The content and uptake of 5-HT by blood platelets in depressive patients. J Neural Transm 45: 285–289.
Post RM, DeLisi LE, Holcomb HH, Uhde TW, Cohen R, Buchsbaum MS (1987). Glucose utilization in the temporal cortex of affectively ill patients: positron emission tomography. Biol Psychiatry 22: 545–553.
Raine A, Buchsbaum M, LaCasse L (1997). Brain abnormalities in murderers indicated by positron emission tomography. Biol Psychiatry 42: 495–508.
Raleigh MJ, Steklis HD, Ervin FR, Kling AS, McGuire MT (1979). The effects of orbitofrontal lesions on the aggressive behavior of vervet monkeys (Cercopithecus aethiops sabaeus). Exp Neurol 66: 158–168.
Siever LJ, Buchsbaum MS, New AS, Spiegel-Cohen J, Wei T, Hazlett EA et al (1999). d,1-Fenfluramine response in impulsive personality disorder assessed with [18F] fluorodeoxyglucose Positron Emission Tomography. Neuropsychopharm 20: 413–423.
Siever LJ, Murphy DL, Slater S, de la Vega E, Lipper S (1984). Plasma prolactin changes following fenfluramine in depressed patients compared to controls: an evaluation of central serotonergic responsivity in depression. Life Sci 34: 1029–1039.
Soloff PH, Meltzer CC, Becker C, Greer PJ, Kelly TM, Constantine D (2003). Impulsivity and prefrontal hypometabolism in borderline personality disorder. Psychiatry Res 123: 153–163.
Soloff PH, Meltzer CC, Greer PJ, Constantine D, Kelly TM (2000). A fenfluramine-activated FDG-PET Study of Borderline Personality Disorder. Biol Psychiatry 47: 540–547.
Spitzer RL, Williams JBW, Gibbon M, First MB (1990). Structured Clinical Interview for DSM-III-R. Patient Edition (SCID-P). American Psychiatric Press: Washington, DC.
Talairach J, Tournoux P (1988). Co-planar Stereotaxic Atlas of the Human Brain. Dimensional Proportional System: An Approach to Cerebral Imaging. Thieme Medical Publishers Inc.: NewYork.
Volkow ND, Tancredi L (1987). Neural substrates of violent behaviour. A preliminary study with positron emission tomography. Br J Psychiatry 151: 668–673.
Woods RP, Cherry SR, Mazziotta JC (1992). Rapid automated algorithm for aligning and reslicing PET images. J Comput Assist Tomogr 16: 620–633.
Zanarini MC, Frankenburg FR, Dubo ED, Sickel AE, Trikha A, Levin A et al (1998). Axis I comorbidity of borderline personality disorder. Am J Psychiatry 155: 1733–1739.
Acknowledgements
We thank Ms Batsheva Halberstam and Dr Dianne Currier for their thoughtful input. Dr Yoram Yovell contributed to the design and funding of the study. This study was supported by NIMH MH40695, American Foundation for Suicide Prevention, NARSAD.
Author information
Authors and Affiliations
Corresponding author
Rights and permissions
About this article
Cite this article
Oquendo, M., Krunic, A., Parsey, R. et al. Positron Emission Tomography of Regional Brain Metabolic Responses to a Serotonergic Challenge in Major Depressive Disorder with and without Borderline Personality Disorder. Neuropsychopharmacol 30, 1163–1172 (2005). https://doi.org/10.1038/sj.npp.1300689
Received:
Revised:
Accepted:
Published:
Issue Date:
DOI: https://doi.org/10.1038/sj.npp.1300689
Keywords
This article is cited by
-
Borderline Personality Disorder and Depression: An Update
Psychiatric Quarterly (2012)
-
Borderline Personality Disorder: Considerations for Inclusion in the Massachusetts Parity List of “Biologically-Based” Disorders
Psychiatric Quarterly (2011)
-
Experiences of Traumatic Events and Associations with PTSD and Depression Development in Urban Health Care-seeking Women
Journal of Urban Health (2008)
